

Feasibility of digital contact tracing in low-income settings - pilot trial for a location-based DCT app
- PMID: 36670358
- PMCID: PMC9859743
- DOI: 10.1186/s12889-022-14888-x
Feasibility of digital contact tracing in low-income settings - pilot trial for a location-based DCT app
Abstract
Background: Data about the effectiveness of digital contact tracing are based on studies conducted in countries with predominantly high- or middle-income settings. Up to now, little research is done to identify specific problems for the implementation of such technique in low-income countries.
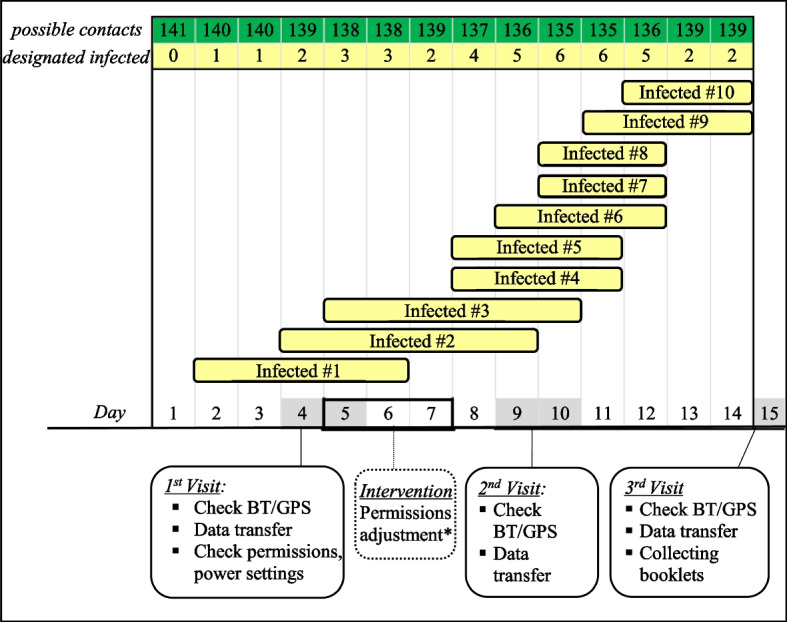
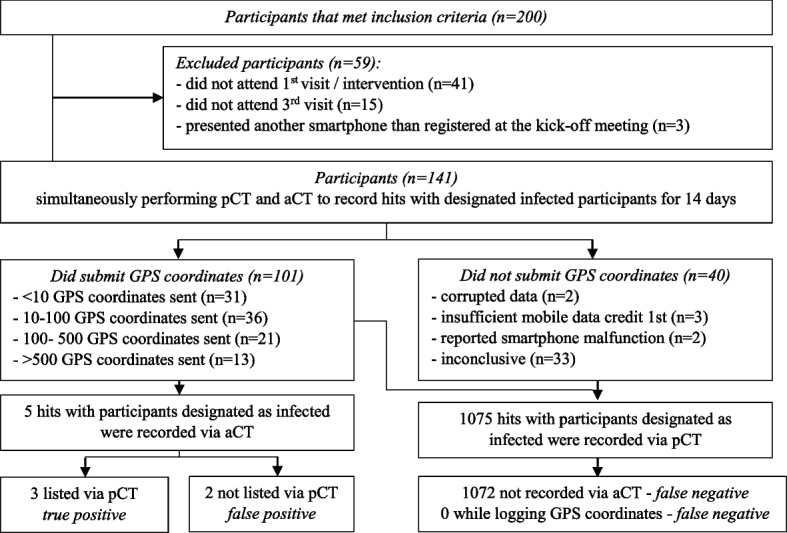
Methods: A Bluetooth-assisted GPS location-based digital contact tracing (DCT) app was tested by 141 participants during 14 days in a hospital in Monrovia, Liberia in February 2020. The DCT app was compared to a paper-based reference system. Hits between participants and 10 designated infected participants were recorded simultaneously by both methods. Additional data about GPS and Bluetooth adherence were gathered and surveys to estimate battery consumption and app adherence were conducted. DCT apps accuracy was evaluated in different settings.
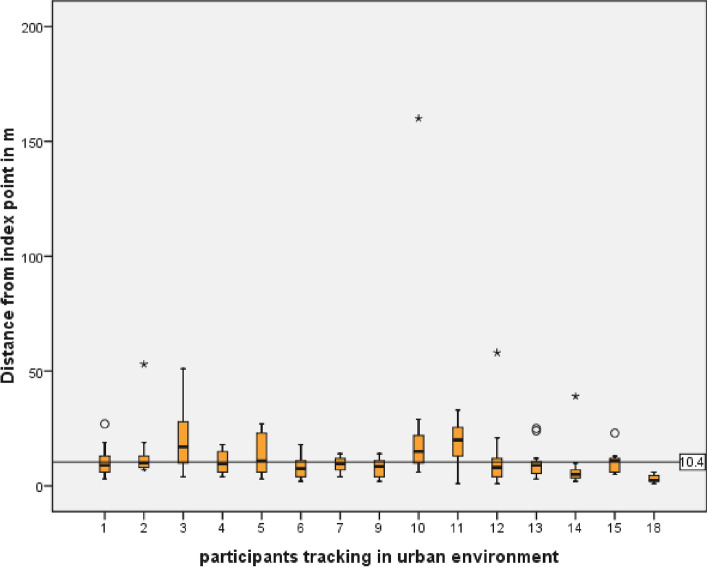
Results: GPS coordinates from 101/141 (71.6%) participants were received. The number of hours recorded by the participants during the study period, true Hours Recorded (tHR), was 496.3 h (1.1% of maximum Hours recordable) during the study period. With the paper-based method 1075 hits and with the DCT app five hits of designated infected participants with other participants have been listed. Differences between true and maximum recording times were due to failed permission settings (45%), data transmission issues (11.3%), of the participants 10.1% switched off GPS and 32.5% experienced other technical or compliance problems. In buildings, use of Bluetooth increased the accuracy of the DCT app (GPS + BT 22.9 m ± 21.6 SD vs. GPS 60.9 m ± 34.7 SD; p = 0.004). GPS accuracy in public transportation was 10.3 m ± 10.05 SD with a significant (p = 0.007) correlation between precision and phone brand. GPS resolution outdoors was 10.4 m ± 4.2 SD.
Conclusion: In our study several limitations of the DCT together with the impairment of GPS accuracy in urban settings impede the solely use of a DCT app. It could be feasible as a supplement to traditional manual contact tracing. DKRS, DRKS00029327 . Registered 20 June 2020 - Retrospectively registered.
Keywords: App; Digital contact tracing; GPS tracking; Location based; Low income; Public health.
© 2023. The Author(s).
Conflict of interest statement
The authors report no competing interest.
Figures






References
-
- WHO global observatory for eHealth, World Health Organization . MHealth: new horizons for health through mobile technologies. Geneva: World Health Organization; 2011.
-
- International Telecommunication Union (ITU) Time series of ICT data for the world, by geographic regions and by level of development. 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
