

Metabolomic Profiling in Patients with Different Hemodynamic Subtypes of Severe Aortic Valve Stenosis
- PMID: 36671480
- PMCID: PMC9855798
- DOI: 10.3390/biom13010095
Metabolomic Profiling in Patients with Different Hemodynamic Subtypes of Severe Aortic Valve Stenosis
Abstract
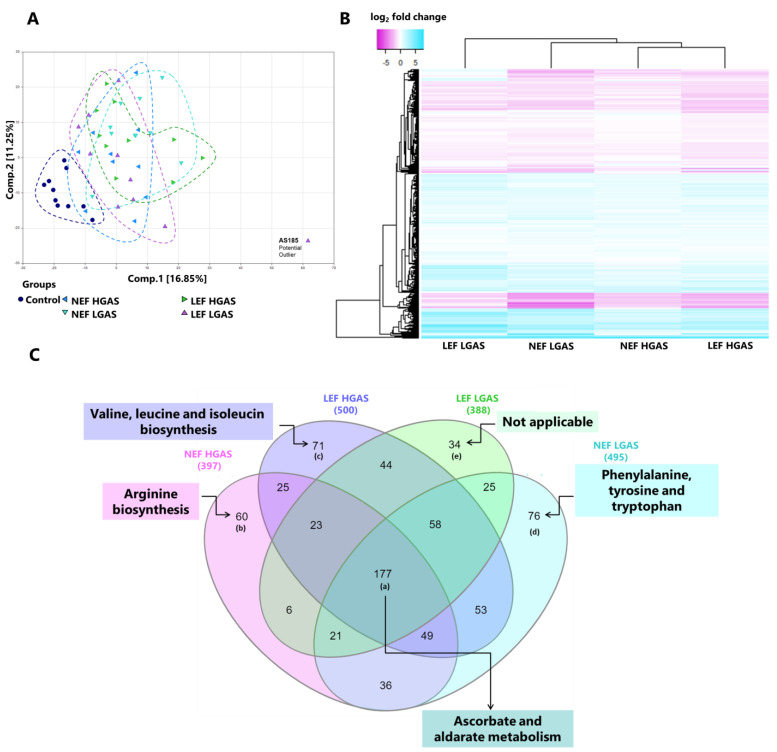
Severe aortic stenosis (AS) is a common pathological condition in an ageing population imposing significant morbidity and mortality. Based on distinct hemodynamic features, i.e., ejection fraction (EF), transvalvular gradient and stroke volume, four different AS subtypes can be distinguished: (i) normal EF and high gradient, (ii) reduced EF and high gradient, (iii) reduced EF and low gradient, and (iv) normal EF and low gradient. These subtypes differ with respect to pathophysiological mechanisms, cardiac remodeling, and prognosis. However, little is known about metabolic changes in these different hemodynamic conditions of AS. Thus, we carried out metabolomic analyses in serum samples of 40 AS patients (n = 10 per subtype) and 10 healthy blood donors (controls) using ultrahigh-performance liquid chromatography-tandem mass spectroscopy. A total of 1293 biochemicals could be identified. Principal component analysis revealed different metabolic profiles in all of the subgroups of AS (All-AS) vs. controls. Out of the determined biochemicals, 48% (n = 620) were altered in All-AS vs. controls (p < 0.05). In this regard, levels of various acylcarnitines (e.g., myristoylcarnitine, fold-change 1.85, p < 0.05), ketone bodies (e.g., 3-hydroxybutyrate, fold-change 11.14, p < 0.05) as well as sugar metabolites (e.g., glucose, fold-change 1.22, p < 0.05) were predominantly increased, whereas amino acids (e.g., leucine, fold-change 0.8, p < 0.05) were mainly reduced in All-AS. Interestingly, these changes appeared to be consistent amongst all AS subtypes. Distinct differences between AS subtypes were found for metabolites belonging to hemoglobin metabolism, diacylglycerols, and dihydrosphingomyelins. These findings indicate that relevant changes in substrate utilization appear to be consistent for different hemodynamic subtypes of AS and may therefore reflect common mechanisms during AS-induced heart failure. Additionally, distinct metabolites could be identified to significantly differ between certain AS subtypes. Future studies need to define their pathophysiological implications.
Keywords: heart failure; hemodynamic subgroups; metabolic remodeling; metabolomics; severe aortic valve stenosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Mack M.J., Leon M.B., Thourani V.H., Makkar R., Kodali S.K., Russo M., Kapadia S.R., Chris Malaisrie S., Cohen D.J., Pibarot P., et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019;380:1695–1705. doi: 10.1056/NEJMoa1814052. - DOI - PubMed
-
- Makkar R.R., Fontana G.P., Jilaihawi H., Kapadia S., Pichard A.D., Douglas P.S., Thourani V.H., Babaliaros V.C., Webb J.G., Herrmann H.C., et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N. Engl. J. Med. 2012;366:1696–1704. doi: 10.1056/NEJMoa1202277. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
