

The Challenges and Prospects of p53-Based Therapies in Ovarian Cancer
- PMID: 36671544
- PMCID: PMC9855757
- DOI: 10.3390/biom13010159
The Challenges and Prospects of p53-Based Therapies in Ovarian Cancer
Abstract
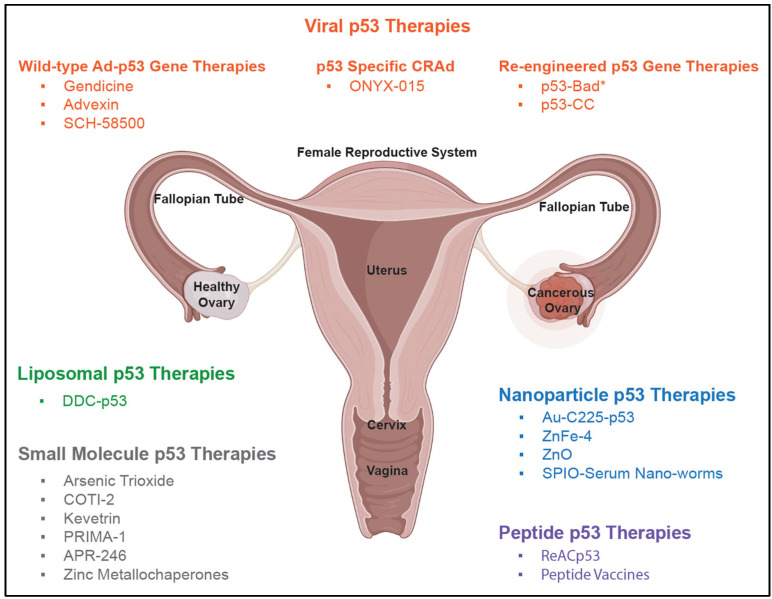
It has been well established that mutations in the tumor suppressor gene, p53, occur readily in a vast majority of cancer tumors, including ovarian cancer. Typically diagnosed in stages three or four, ovarian cancer is the fifth leading cause of death in women, despite accounting for only 2.5% of all female malignancies. The overall 5-year survival rate for ovarian cancer is around 47%; however, this drops to an abysmal 29% for the most common type of ovarian cancer, high-grade serous ovarian carcinoma (HGSOC). HGSOC has upwards of 96% of cases expressing mutations in p53. Therefore, wild-type (WT) p53 and p53-based therapies have been explored as treatment options via a plethora of drug delivery vehicles including nanoparticles, viruses, polymers, and liposomes. However, previous p53 therapeutics have faced many challenges, which have resulted in their limited translational success to date. This review highlights a selection of these historical p53-targeted therapeutics for ovarian cancer, why they failed, and what the future could hold for a new generation of this class of therapies.
Keywords: HGSOC; gene delivery; gene therapy; ovarian cancer; p53 therapies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
