

Poor Internal Jugular Venous Outflow Is Associated with Poor Cortical Venous Outflow and Outcomes after Successful Endovascular Reperfusion Therapy
- PMID: 36672011
- PMCID: PMC9856844
- DOI: 10.3390/brainsci13010032
Poor Internal Jugular Venous Outflow Is Associated with Poor Cortical Venous Outflow and Outcomes after Successful Endovascular Reperfusion Therapy
Abstract
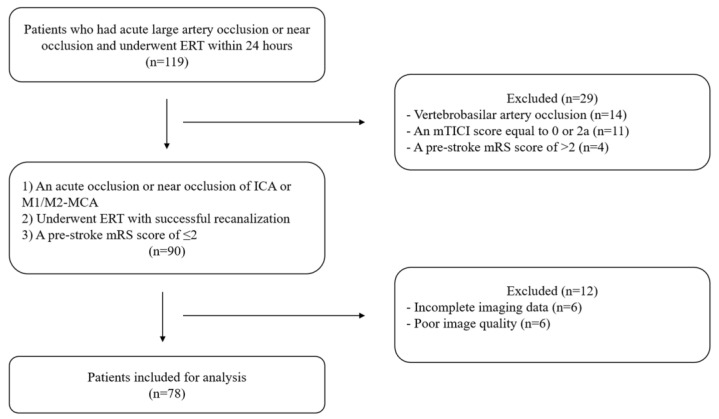
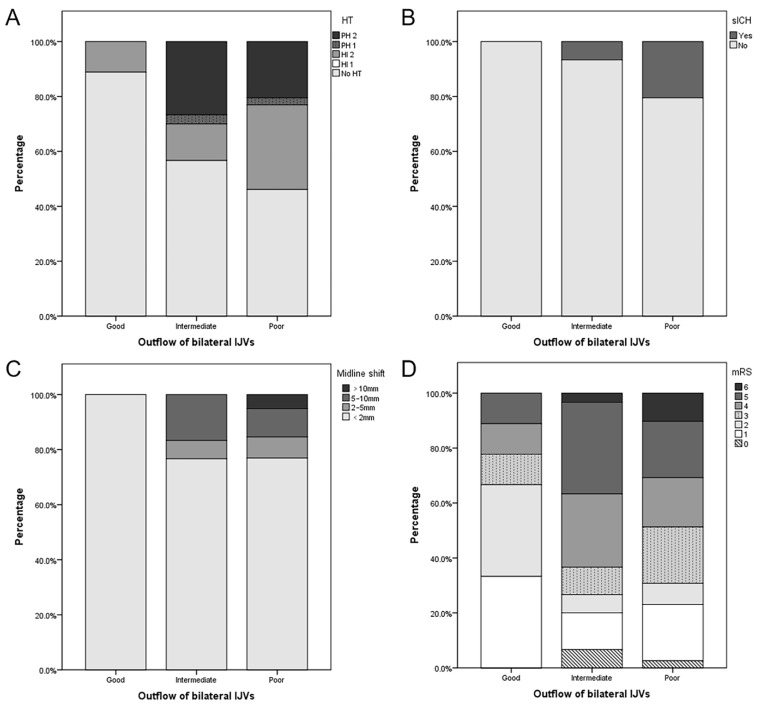
Many patients show poor outcomes following endovascular reperfusion therapy (ERT), and poor cortical venous outflow is a risk factor for these poor outcomes. We investigated the association between the outflow of the internal jugular vein (IJV) and baseline cortical venous outflow and the outcomes after ERT. We retrospectively enrolled 78 patients diagnosed with an acute anterior circulation stroke and successful ERT. Poor IJV outflow on the affected side was defined as stenosis ≥50% or occlusion of ipsilateral IJV, and poor outflow of bilateral IJVs was defined as stenosis ≥50% or occlusion of both IJVs. Poor cortical venous outflow was defined as a cortical vein opacification score (COVES) of 0 on admission. Multivariate analysis showed that poor outflow of IJV on the affected side was an independent predictor for hemorrhagic transformation. The poor outflow of bilateral IJVs was an independent risk factor for poor clinical outcomes. These patients also had numerical trends of a higher incidence of symptomatic intracranial hemorrhage, midline shift >10 mm, and in-hospital mortality; however, statistical significance was not observed. Additionally, poor IJV outflow was an independent determinant of poor cortical venous outflow. For acute large vessel occlusion patients, poor IJV outflow is associated with poor baseline cortical venous outflow and outcomes after successful ERT.
Keywords: angiography; endovascular reperfusion therapy; prognosis; stroke; venous flow.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Goyal M., Menon B.K., van Zwam W.H., Dippel D.W.J., Mitchell P.J., Demchuk A.M., Dávalos A., Majoie C.B.L.M., Van Der Lugt A., De Miquel M.A., et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
Grants and funding
- 2020B1212060017/Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases
- 2020B1111170002/Guangdong Provincial Clinical Research Center for Neurological Diseases
- 2015B050501003 and 2020A0505020004/Southern China International Joint Research Center for Early Intervention and Functional Rehabilitation of Neurological Diseases
- 201604020010/Guangdong Provincial Engineering Center for Major Neurological Disease Treatment, Guangdong Provincial Translational Medicine Innovation Platform for Diagnosis and Treatment of Major Neurological Disease, Guangzhou Clinical Research and Translational Cent
LinkOut - more resources
Full Text Sources
