

Pathophysiology of Inflammatory Bowel Disease: Innate Immune System
- PMID: 36675038
- PMCID: PMC9863490
- DOI: 10.3390/ijms24021526
Pathophysiology of Inflammatory Bowel Disease: Innate Immune System
Abstract
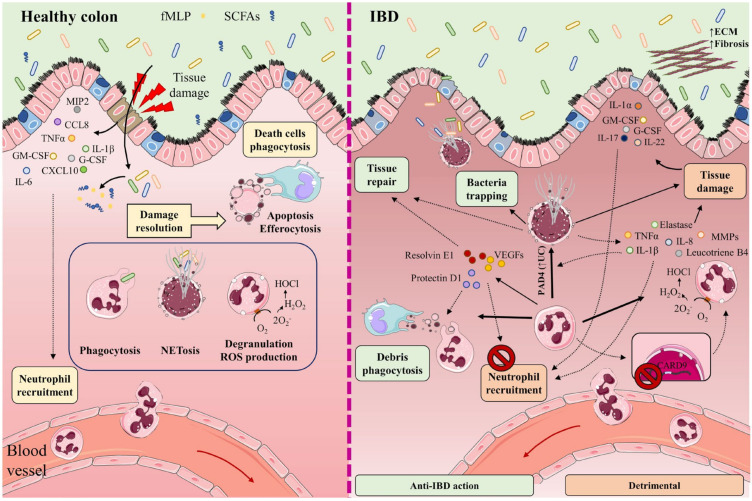
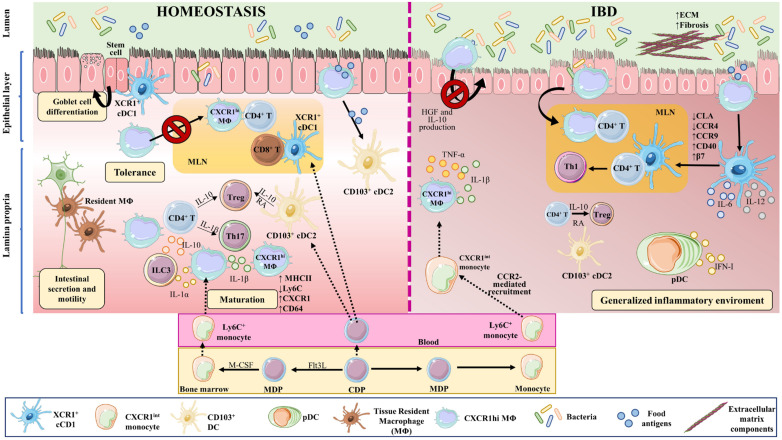
Inflammatory bowel disease (IBD), comprising Crohn's disease (CD) and ulcerative colitis (UC), is a heterogeneous state of chronic intestinal inflammation with no exact known cause. Intestinal innate immunity is enacted by neutrophils, monocytes, macrophages, and dendritic cells (DCs), and innate lymphoid cells and NK cells, characterized by their capacity to produce a rapid and nonspecific reaction as a first-line response. Innate immune cells (IIC) defend against pathogens and excessive entry of intestinal microorganisms, while preserving immune tolerance to resident intestinal microbiota. Changes to this equilibrium are linked to intestinal inflammation in the gut and IBD. IICs mediate host defense responses, inflammation, and tissue healing by producing cytokines and chemokines, activating the complement cascade and phagocytosis, or presenting antigens to activate the adaptive immune response. IICs exert important functions that promote or ameliorate the cellular and molecular mechanisms that underlie and sustain IBD. A comprehensive understanding of the mechanisms underlying these clinical manifestations will be important for developing therapies targeting the innate immune system in IBD patients. This review examines the complex roles of and interactions among IICs, and their interactions with other immune and non-immune cells in homeostasis and pathological conditions.
Keywords: Crohn’s disease; dendritic cell; inflammatory bowel disease; innate immune system; intestinal homeostasis; macrophage; neutrophil; ulcerative colitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Levine A., Griffiths A., Markowitz J., Wilson D.C., Turner D., Russell R.K., Fell J., Ruemmele F.M., Walters T., Sherlock M., et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011;17:1314–1321. doi: 10.1002/ibd.21493. - DOI - PubMed
-
- Molodecky N.A., Soon I.S., Rabi D.M., Ghali W.A., Ferris M., Chernoff G., Benchimol E.I., Panaccione R., Ghosh S., Barkema H.W., et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54.e42. doi: 10.1053/j.gastro.2011.10.001. quiz e30. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
