

Crohn's Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities
- PMID: 36675403
- PMCID: PMC9860571
- DOI: 10.3390/jcm12020466
Crohn's Disease-Associated and Cryptoglandular Fistulas: Differences and Similarities
Abstract
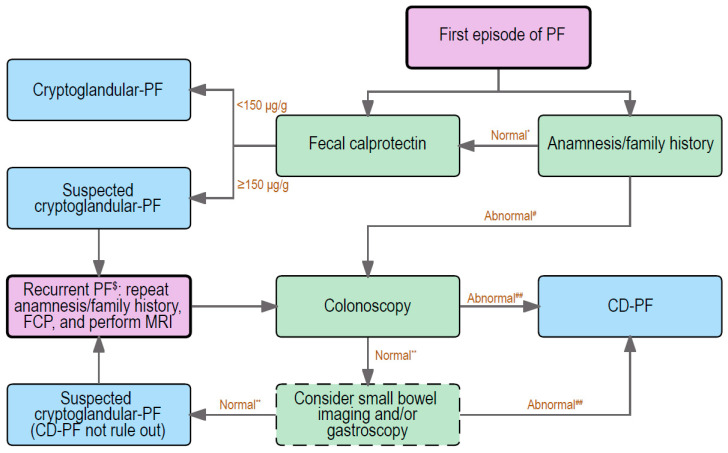
Perianal fistulas are defined as pathological connections between the anorectal canal and the perianal skin. Most perianal fistulas are cryptoglandular fistulas, which are thought to originate from infected anal glands. The remainder of the fistulas mainly arises as complications of Crohn's disease (CD), trauma, or as a result of malignancies. Fistulas in CD are considered as a consequence of a chronic and transmural inflammatory process in the distal bowel and can, in some cases, even precede the diagnosis of CD. Although both cryptoglandular and CD-associated fistulas might look similar macroscopically, they differ considerably in their complexity, treatment options, and healing rate. Therefore, it is of crucial importance to differentiate between these two types of fistulas. In this review, the differences between CD-associated and cryptoglandular perianal fistulas in epidemiology, pathogenesis, and clinical management are discussed. Finally, a flow chart is provided for physicians to guide them when dealing with patients displaying their first episode of perianal fistulas.
Keywords: Crohn’s disease; clinical practice; cryptoglandular fistulas; differences and similarities; perianal fistulas.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- de Miguel Criado J., del Salto L.G., Rivas P.F., del Hoyo L.F., Velasco L.G., de las Vacas M.I., Marco Sanz A.G., Paradela M.M., Moreno E.F. MR imaging evaluation of perianal fistulas: Spectrum of imaging features. Radiogr. A Rev. Publ. Radiol. Soc. N. Am. Inc. 2012;32:175–194. doi: 10.1148/rg.321115040. - DOI - PubMed
-
- Gottgens K.W., Jeuring S.F., Sturkenboom R., Romberg-Camps M.J., Oostenbrug L.E., Jonkers D.M., Stassen L.P., Masclee A.A., Pierik M.J., Breukink S.O. Time trends in the epidemiology and outcome of perianal fistulizing Crohn’s disease in a population-based cohort. Eur. J. Gastroenterol. Hepatol. 2017;29:595–601. doi: 10.1097/MEG.0000000000000840. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
