

Novel Machine Learning Approach to Predict and Personalize Length of Stay for Patients Admitted with Syncope from the Emergency Department
- PMID: 36675668
- PMCID: PMC9864075
- DOI: 10.3390/jpm13010007
Novel Machine Learning Approach to Predict and Personalize Length of Stay for Patients Admitted with Syncope from the Emergency Department
Abstract
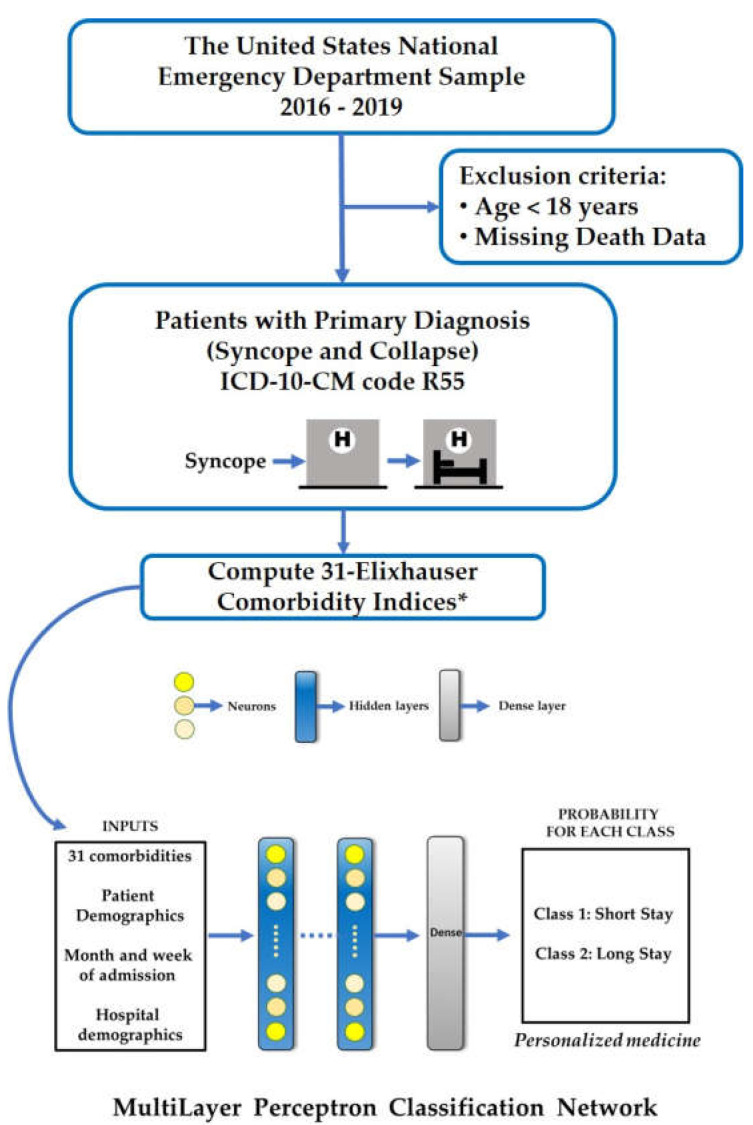
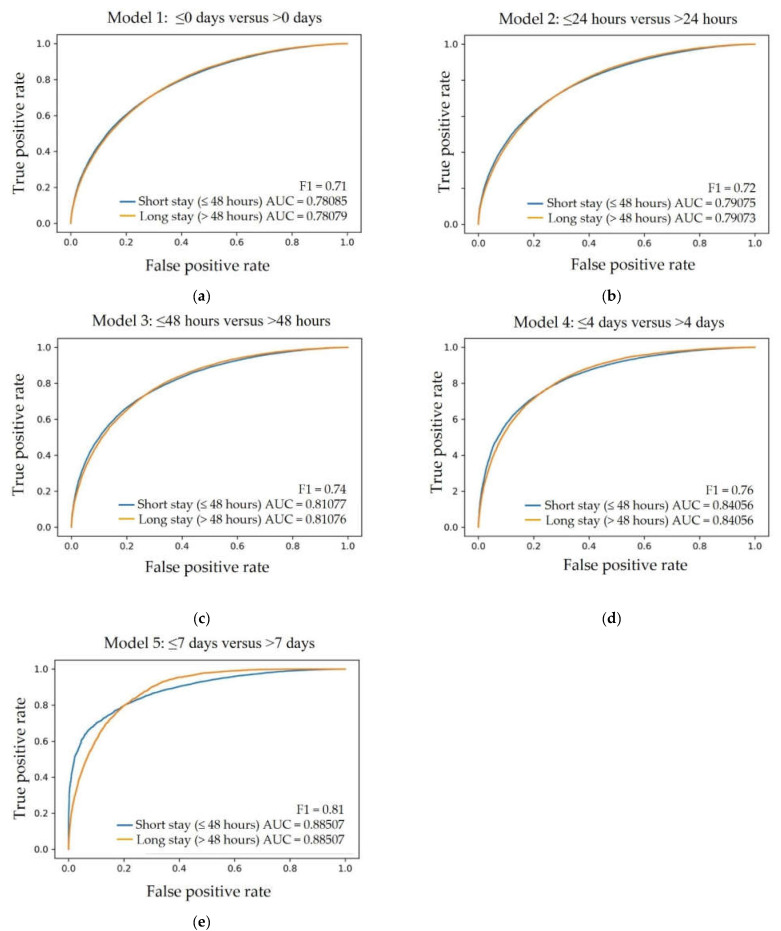
Background: Syncope, a common problem encountered in the emergency department (ED), has a multitude of causes ranging from benign to life-threatening. Hospitalization may be required, but the management can vary substantially depending on specific clinical characteristics. Models predicting admission and hospitalization length of stay (LoS) are lacking. The purpose of this study was to design an effective, exploratory model using machine learning (ML) technology to predict LoS for patients presenting with syncope. Methods: This was a retrospective analysis using over 4 million patients from the National Emergency Department Sample (NEDS) database presenting to the ED with syncope between 2016−2019. A multilayer perceptron neural network with one hidden layer was trained and validated on this data set. Results: Receiver Operator Characteristics (ROC) were determined for each of the five ANN models with varying cutoffs for LoS. A fair area under the curve (AUC of 0.78) to good (AUC of 0.88) prediction performance was achieved based on sequential analysis at different cutoff points, starting from the same day discharge and ending at the longest analyzed cutoff LoS ≤7 days versus >7 days, accordingly. The ML algorithm showed significant sensitivity and specificity in predicting short (≤48 h) versus long (>48 h) LoS, with an AUC of 0.81. Conclusions: Using variables available to triaging ED clinicians, ML shows promise in predicting hospital LoS with fair to good performance for patients presenting with syncope.
Keywords: artificial intelligence; length of stay; machine learning; prediction; syncope.
Conflict of interest statement
M.S. is an inventor on patents and patent applications in computer vision and medical image analysis. He is a co-founder of Medical Imaging Applications, LLC, Coralville, Iowa, USA and VIDA Diagnostics, Inc., Coralville, Iowa, USA. B.O. serves on the DSMB for Astra Zeneca. The authors S.L., A.R.M., D.K.P., M.A., E.J.B., G.M.S., T.B., S.L.J., A.Z.E. and M.A.G. declare no conflict of interest.
Figures
References
-
- Sheldon R.S., Morillo C.A., Krahn A.D., O'Neill B., Thiruganasambandamoorthy V., Parkash R., Talajic M., Tu J.V., Seifer C., Johnstone D., et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can. J. Cardiol. 2011;27:246–253. doi: 10.1016/j.cjca.2010.11.002. - DOI - PubMed
-
- Dipaola F., Gatti M., Pacetti V., Bottaccioli A.G., Shiffer D., Minonzio M., Mene R., Giaj Levra A., Solbiati M., Costantino G., et al. Artificial Intelligence Algorithms and Natural Language Processing for the Recognition of Syncope Patients on Emergency Department Medical Records. J. Clin. Med. 2019;8:1677. doi: 10.3390/jcm8101677. - DOI - PMC - PubMed
-
- Writing Committee M., Shen W.K., Sheldon R.S., Benditt D.G., Cohen M.I., Forman D.E., Goldberger Z.D., Grubb B.P., Hamdan M.H., Krahn A.D., et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. 2017;14:e155–e217. doi: 10.1016/j.hrthm.2017.03.004. - DOI - PubMed
LinkOut - more resources
Full Text Sources
