

Developments in Combining Targeted Radionuclide Therapies and Immunotherapies for Cancer Treatment
- PMID: 36678756
- PMCID: PMC9865370
- DOI: 10.3390/pharmaceutics15010128
Developments in Combining Targeted Radionuclide Therapies and Immunotherapies for Cancer Treatment
Abstract
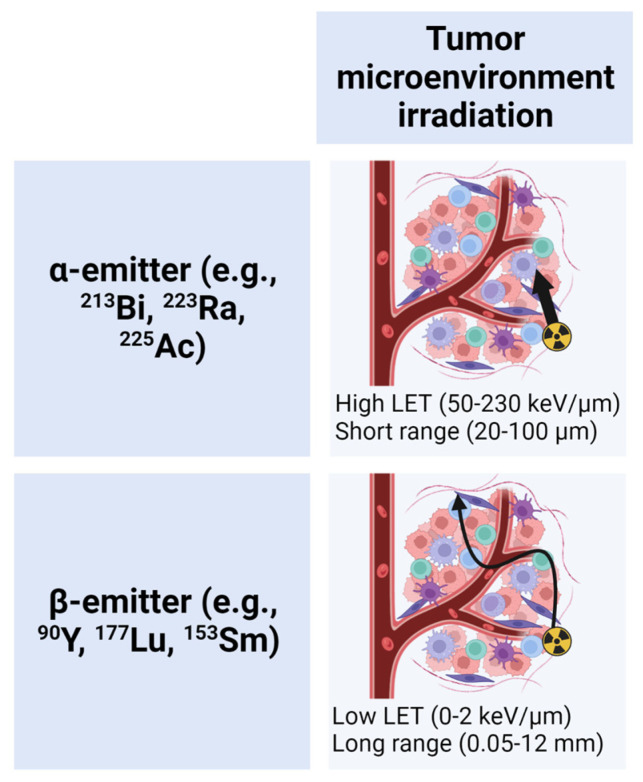
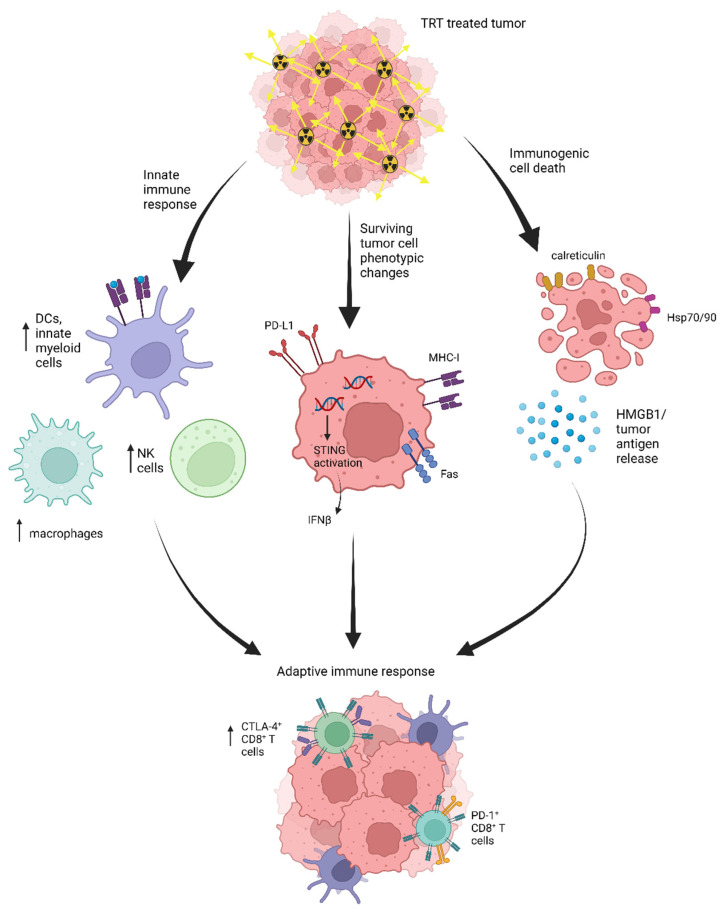
Targeted radionuclide therapy (TRT) and immunotherapy are rapidly growing classes of cancer treatments. Basic, translational, and clinical research are now investigating therapeutic combinations of these agents. In comparison to external beam radiation therapy (EBRT), TRT has the unique advantage of treating all disease sites following intravenous injection and selective tumor uptake and retention-a particularly beneficial property in metastatic disease settings. The therapeutic value of combining radiation therapy with immune checkpoint blockade to treat metastases has been demonstrated in preclinical studies, whereas results of clinical studies have been mixed. Several clinical trials combining TRT and immune checkpoint blockade have been initiated based on preclinical studies combining these with EBRT and/or TRT. Despite the interest in translation of TRT and immunotherapy combinations, many questions remain surrounding the mechanisms of interaction and the optimal approach to clinical implementation of these combinations. This review highlights the mechanisms of interaction between anti-tumor immunity and radiation therapy and the status of basic and translational research and clinical trials investigating combinations of TRT and immunotherapies.
Keywords: anti-tumor immunity; external beam radiation therapy (EBRT); targeted radionuclide therapy (TRT); tumor microenvironment (TME).
Conflict of interest statement
J.J.G. is the cofounder and Chief Innovation Officer of Voximetry, Inc. J.P.W. is a founder and Chief Science Advisor for Archeus Technologies, which holds the license rights to NM600 related technologies. Z.S.M. is a member of the scientific advisory board for Seneca Therapeutics and Archeus Technologies.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
