

Advances in Antibody-Based Therapeutics for Cerebral Ischemia
- PMID: 36678774
- PMCID: PMC9866586
- DOI: 10.3390/pharmaceutics15010145
Advances in Antibody-Based Therapeutics for Cerebral Ischemia
Abstract
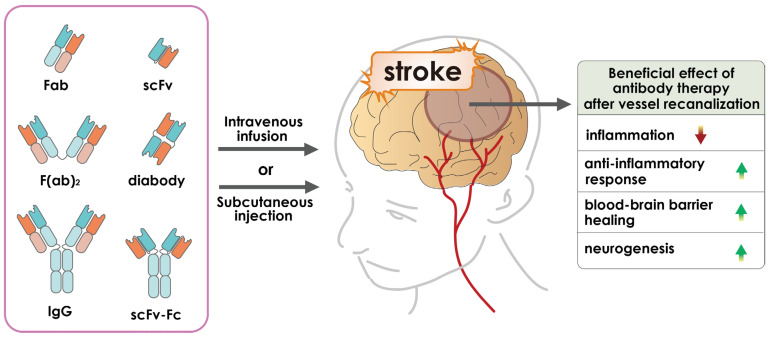
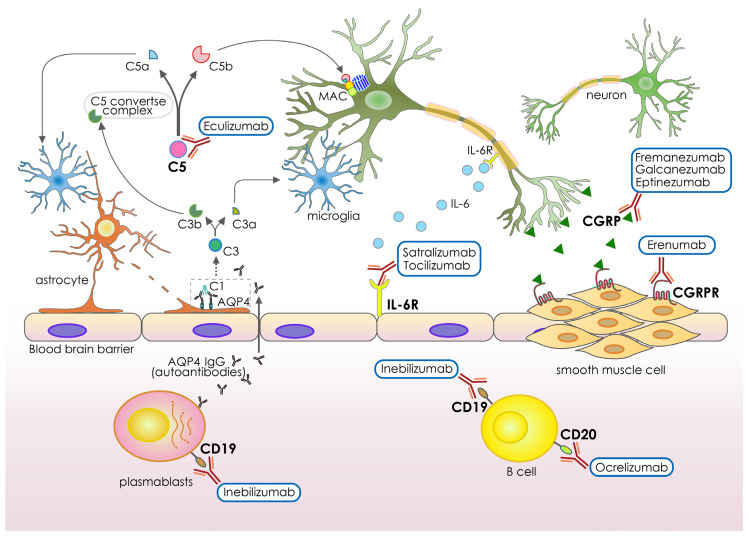
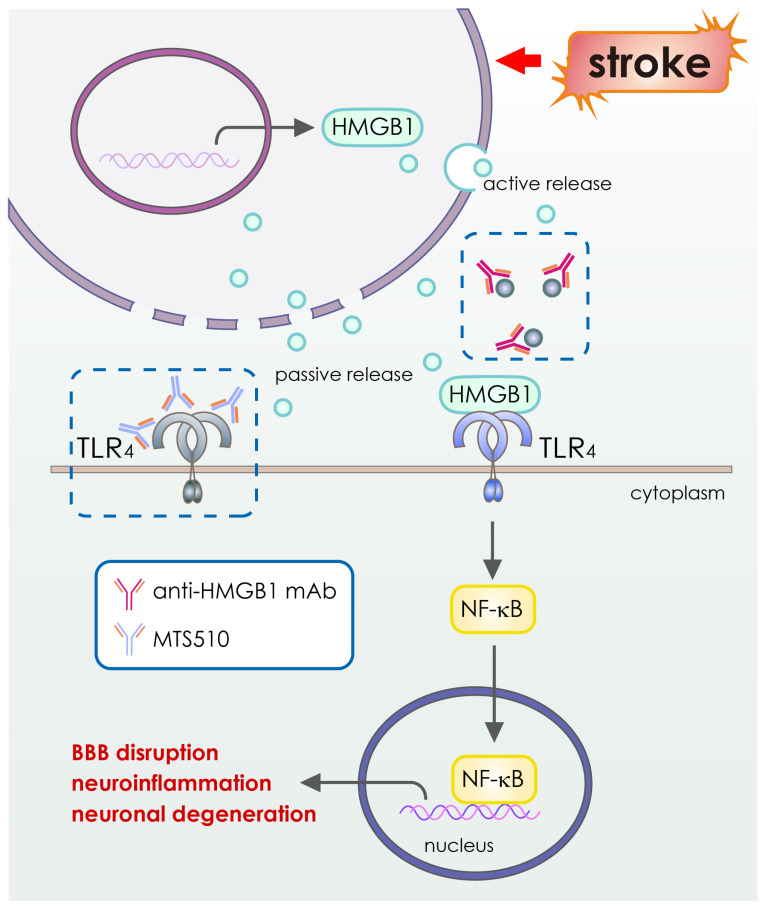
Cerebral ischemia is an acute disorder characterized by an abrupt reduction in blood flow that results in immediate deprivation of both glucose and oxygen. The main types of cerebral ischemia are ischemic and hemorrhagic stroke. When a stroke occurs, several signaling pathways are activated, comprising necrosis, apoptosis, and autophagy as well as glial activation and white matter injury, which leads to neuronal cell death. Current treatments for strokes include challenging mechanical thrombectomy or tissue plasminogen activator, which increase the danger of cerebral bleeding, brain edema, and cerebral damage, limiting their usage in clinical settings. Monoclonal antibody therapy has proven to be effective and safe in the treatment of a variety of neurological disorders. In contrast, the evidence for stroke therapy is minimal. Recently, Clone MTS510 antibody targeting toll-like receptor-4 (TLR4) protein, ASC06-IgG1 antibody targeting acid sensing ion channel-1a (ASIC1a) protein, Anti-GluN1 antibodies targeting N-methyl-D-aspartate (NMDA) receptor associated calcium influx, GSK249320 antibody targeting myelin-associated glycoprotein (MAG), anti-High Mobility Group Box-1 antibody targeting high mobility group box-1 (HMGB1) are currently under clinical trials for cerebral ischemia treatment. In this article, we review the current antibody-based pharmaceuticals for neurological diseases, the use of antibody drugs in stroke, strategies to improve the efficacy of antibody therapeutics in cerebral ischemia, and the recent advancement of antibody drugs in clinical practice. Overall, we highlight the need of enhancing blood-brain barrier (BBB) penetration for the improvement of antibody-based therapeutics in the brain, which could greatly enhance the antibody medications for cerebral ischemia in clinical practice.
Keywords: antibody; blood brain barrier; cerebral ischemia; hemorrhagic; ischemic.
Conflict of interest statement
All the authors have no conflict of interest to declare.
Figures





References
-
- Owolabi M.O., Akarolo-Anthony S., Akinyemi R., Arnett D., Gebregziabher M., Jenkins C., Tiwari H., Arulogun O., Akpalu A., Sarfo F.S., et al. The burden of stroke in Africa: A glance at the present and a glimpse into the future. Cardiovasc. J. Afr. 2015;26:S27–S38. doi: 10.5830/CVJA-2015-038. - DOI - PMC - PubMed
-
- Chakroun-Walha O., Samet A., Ben Abdallah M., Benmansour S., Issaoui F., Rebai M., Ben Messaoud K., Benali C., Mokni W., Nasri A., et al. Stroke knowledge among emergency centre visitors: A cross-sectional multicenter survey. Afr. J. Emerg. Med. 2021;11:10–14. doi: 10.1016/j.afjem.2020.10.012. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
