

A Cost-Effectiveness Analysis of Pre-Exposure Prophylaxis to Avert Rabies Deaths in School-Aged Children in India
- PMID: 36679933
- PMCID: PMC9866950
- DOI: 10.3390/vaccines11010088
A Cost-Effectiveness Analysis of Pre-Exposure Prophylaxis to Avert Rabies Deaths in School-Aged Children in India
Abstract
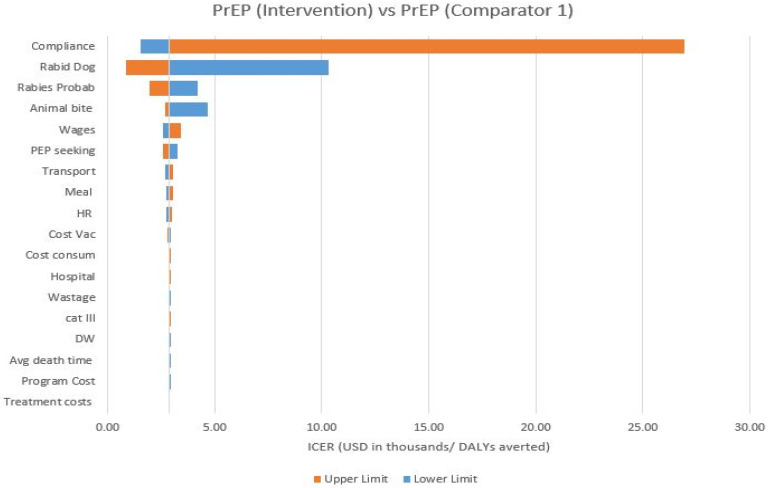
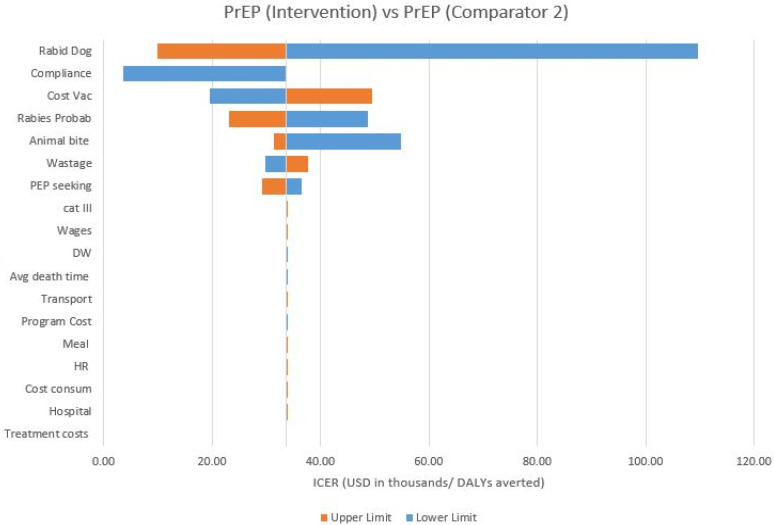
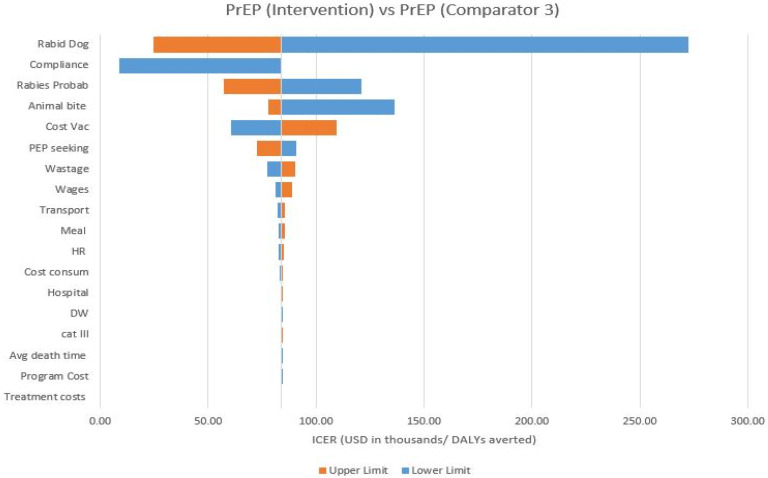
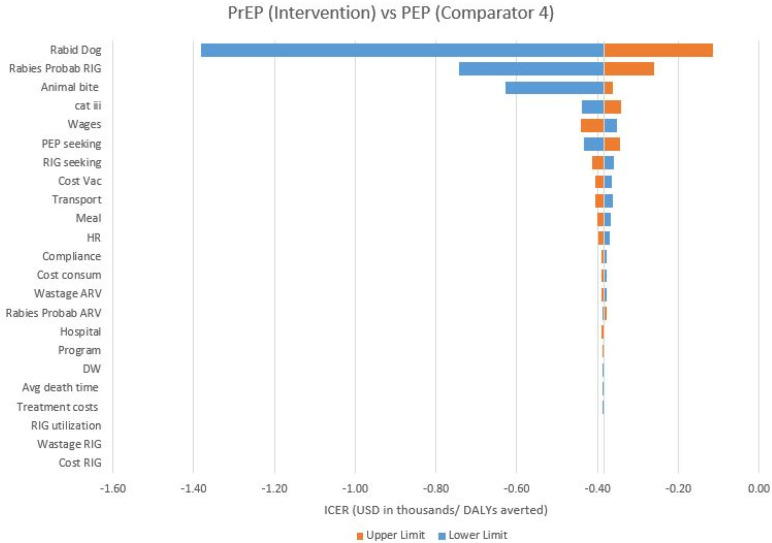
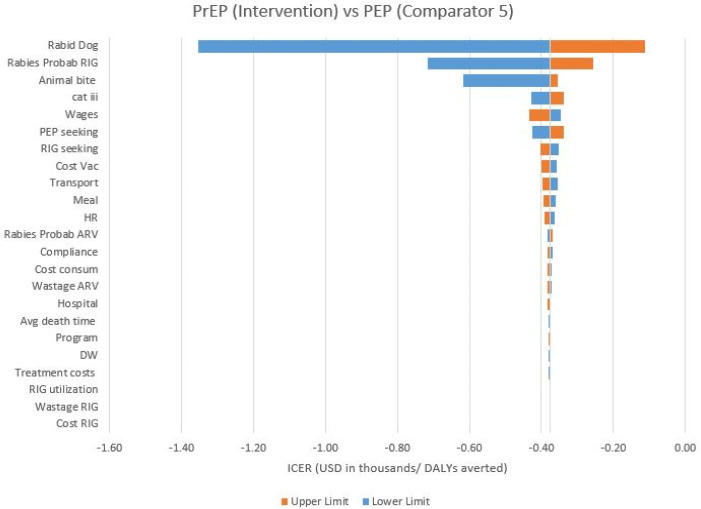
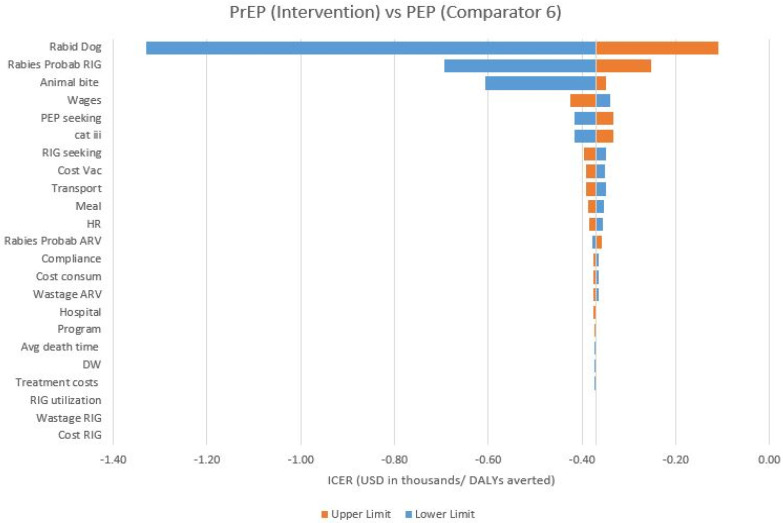
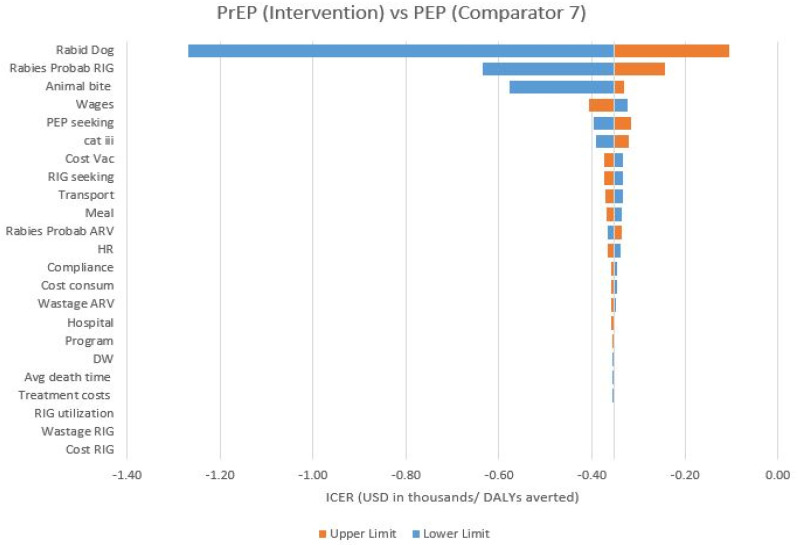
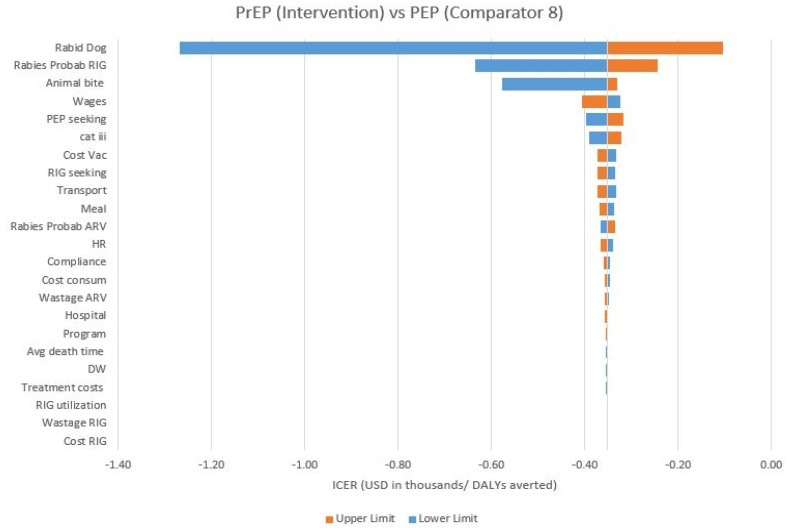
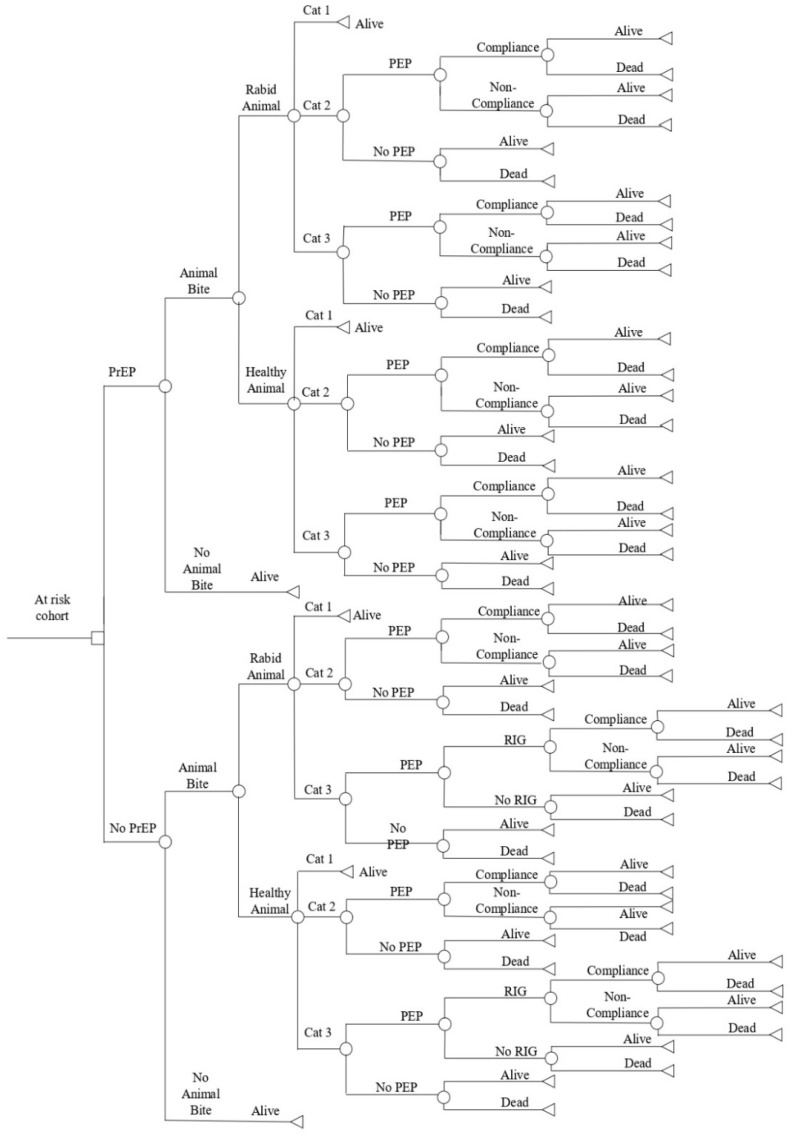
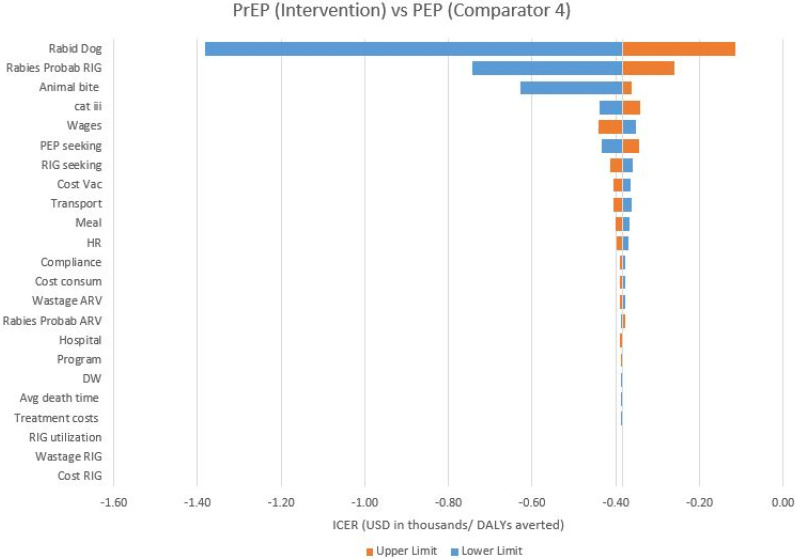
Children contribute to one-half of the total painful rabies mortalities in India. The state-of-the-art rabies mortality averting strategies need exploration for the effective implementation of pre-exposure prophylaxis (PrEP) in India. This study reports on the economic evaluation of various PrEP and post-exposure prophylaxis (PEP) strategies to avert rabies mortalities in school-aged children in India. A decision tree model has been developed for children in the age group of 5-15 years to evaluate various PrEP + PEP and PEP only regimens. The 2-site intradermal regimen administered on day zero and seven was chosen as the intervention [PrEP (I)]. ICER was calculated from the quasi-societal and quasi-health systems' perspectives for the base case analysis, along with one-way sensitivity, and scenario analyses for each regimen. The incremental DALYs averted per million population with the implementation of PrEP (I) ranged between 451 and 85,069 in 2020. The ICER was reported in the range of USD 384-352/DALY averted (non-dominant) in comparison to PEP regimens from a quasi-societal perspective. PrEP (I) is reported to be 'very cost effective' in comparison with PEP regimens from the quasi-societal and quasi-health systems' perspectives and reduce deaths by up to 89.9%. This study concludes that the PrEP (I) regimen is a cost-effective and life-saving strategy to avert painful mortalities due to rabies in school-aged children in India.
Keywords: India; child health; cost effectiveness; public health; rabies; school-aged children.
Conflict of interest statement
Omesh Bharti is a rabies expert and is currently affiliated with the State Epidemiologist in State Institute of Health and Family Welfare, Department of Health & Family Welfare, Government of Himachal Pradesh, Shimla, India. He has contributed to the conceptualization of the study, provided an expert opinion, contributed to the development and validation of the decision tree model, and reviewed the final manuscript. The publication of the study results was not contingent on the sponsor’s approval or censorship of the manuscript.
Figures
References
-
- WHO Expert Consultation on Rabies, Third Report. World Health Organization; Geneva, Switzerland: 2018. (WHO Technical Report Series, No.1012).
-
- Sudarshan M.K., Madhusudana S.N., Mahendra B.J., Rao N.S., Ashwath Narayana D.H., Abdul Rahman S., Meslin F.-X., Lobo D., Ravikumar K., Gangaboraiah. Assessing the burden of human rabies in India: Results of a national multi-center epidemiological survey. Int. J. Infect. Dis. 2007;11:29–35. doi: 10.1016/j.ijid.2005.10.007. - DOI - PubMed
-
- Sudarshan M.K., Madhusudana S.N., Mahendra B.J., Rao N.S.N., Ashwath Narayana D.H., Abdul Rahman S., Meslin F.-X., Lobo D., Ravikumar G.K. Indian Multicentric Rabies Survey 2017; World Health Organization—Association for Prevention and Control of Rabies in India (APRCI), India 2018. [(accessed on 22 December 2022)]. Available online: https://fctc.who.int/publications/i/item/world-health-organization---ass....
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
