

Prediction of conduction disturbances in patients undergoing transcatheter aortic valve replacement
- PMID: 36680617
- PMCID: PMC10160192
- DOI: 10.1007/s00392-023-02160-0
Prediction of conduction disturbances in patients undergoing transcatheter aortic valve replacement
Abstract
Aim: Transcatheter aortic valve replacement (TAVR) can cause intraventricular conduction disturbances (ICA), particularly left bundle branch block (BBB) and high-degree atrioventricular block (HAVB). The aim of this study was to investigate clinical, anatomical, procedural, and electrophysiological parameters predicting ICA after TAVR.
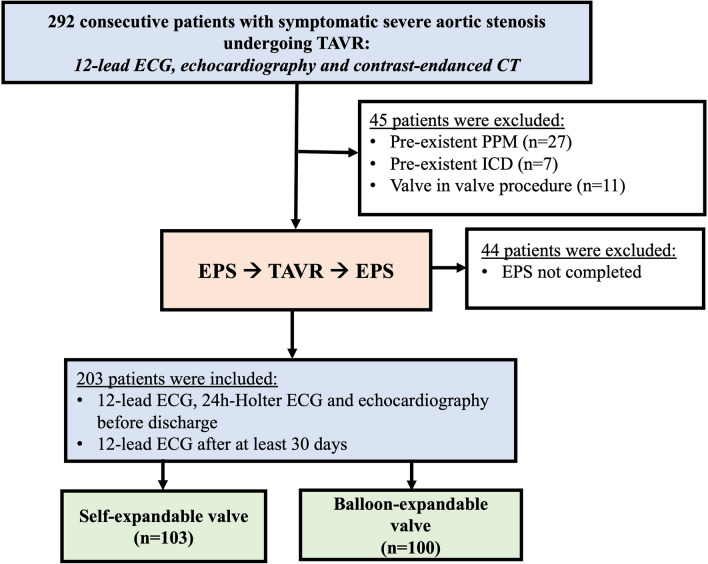
Methods: Patients with severe aortic stenosis (n = 203) without pacing devices undergoing TAVR with a self-expanding (n = 103) or balloon-expanding (n = 100) valve were enrolled. Clinical and anatomical parameters, such as length of the membranous septum (MS) and implantation depth, were assessed. His-ventricular interval (HVi) before and after implantation was determined. 12-lead-electrocardiograms (ECG) before, during and after 3 and 30 days after TAVR were analyzed for detection of any ICA.
Results: Among 203 consecutive patients (aortic valve area 0.78 ± 0.18 cm2, age 80 ± 6 years, 54% male, left ventricular ejection fraction 52 ± 10%), TAVR led to a significant prolongation of infranodal conduction in all patients from 49 ± 10 ms to 59 ± 16 ms (p = 0.01). The HVi prolongation was independent of valve types, occurrence of HAVB or ICA. Fifteen patients (7%) developed HAVB requiring permanent pacemaker (PPM) implantation and 63 patients (31%) developed ICA within 30 days. Pre-existing BBB (OR 11.64; 95% CI 2.87-47.20; p = 0.001), new-onset left BBB (OR 15.72; 95% CI 3.05-81.03; p = 0.001), and diabetes mellitus (OR 3.88; 95% CI 1.30-15.99; p = 0.02) independently predicted HAVB requiring PPM. Neither pre-existing right BBB, a prolonged postHVi, increases in PR duration, any of the TAVR implantation procedural and anatomic nor echocardiographic characteristics were predictive for later HAVB.
Conclusions: New-onset left BBB and diabetes mellitus independently predicted HAVB requiring PPM after TAVR and helped to identify patients at risk. Electrophysiologic study (EPS) of atrioventricular conduction was neither specific nor predictive of HAVB and can be skipped.
Trial registration number: NCT04128384 ( https://www.
Clinicaltrials: gov ).
Keywords: Conduction disturbances; Transcatheter valve replacement.
© 2023. The Author(s).
Conflict of interest statement
FM has received scientific support and speaker honoraria from Bayer, Boehringer Ingelheim, Medtronic, and ReCor Medical. SE has received speaker honoraria from Medtronic, Recor, Bayer, Daiichi Sankyo, Novartis, AstraZeneca, Akcea Therapeutics and Pfizer. MB has received scientific support and speaker honoraria from Abbot, Amgen, Bayer, Boehringer Ingelheim, Medtronic, Novartis, Servier and ReCor Medical. CU has received scientific support and speaker Honoria from Bayer, Pfizer, Medtronic, and ReCor Medical. All other authors have no conflict of interest to report.
Figures

References
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Rev Esp Cardiol (Engl Ed). 2022;75(6):524. doi: 10.1016/j.rec.2022.05.006. - DOI - PubMed
-
- Siontis GC, Praz F, Pilgrim T, Mavridis D, Verma S, Salanti G, Søndergaard L, Jüni P, Windecker S. Transcatheter aortic valve implantation vs surgical aortic valve replacement for treatment of severe aortic stenosis: a meta-analysis of randomized trials. Eur Heart J. 2016;37(47):3503–3512. doi: 10.1093/eurheartj/ehw225. - DOI - PubMed
-
- Leon MB, Mack MJ, Hahn RT, Thourani VH, Makkar R, Kodali SK, Alu MC, Madhavan MV, Chau KH, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Blanke P, Leipsic JA, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Herrmann HC, Szeto WY, Genereux P, Pershad A, Lu M, Webb JG, Smith CR, Pibarot P. Outcomes 2 years after transcatheter aortic valve replacement in patients at low surgical risk. J Am Coll Cardiol. 2021;77(9):1149–1161. doi: 10.1016/j.jacc.2020.12.052. - DOI - PubMed
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42(35):3427–3520. doi: 10.1093/eurheartj/ehab364. - DOI - PubMed
-
- Urena M, Mok M, Serra V, Dumont E, Nombela-Franco L, DeLarochellière R, Doyle D, Igual A, Larose E, Amat-Santos I, Côté M, Cuéllar H, Pibarot P, de Jaegere P, Philippon F, Garcia del Blanco B, Rodés-Cabau J. Predictive factors and long-term clinical consequences of persistent left bundle branch block following transcatheter aortic valve implantation with a balloon-expandable valve. J Am Coll Cardiol. 2012;60(18):1743–1752. doi: 10.1016/j.jacc.2012.07.035. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
