

Operative and long-term outcomes of combined and staged carotid endarterectomy and coronary bypass
- PMID: 36681256
- PMCID: PMC10353412
- DOI: 10.1016/j.jvs.2023.01.015
Operative and long-term outcomes of combined and staged carotid endarterectomy and coronary bypass
Abstract
Objective: Optimal temporal surgical management of significant carotid stenosis and coronary artery disease remains unknown. Carotid endarterectomy (CEA) and coronary artery bypass (CABG) are performed concurrently (CCAB) or in a staged (CEA-CABG or CABG-CEA) approach. Using the Vascular Quality Initiative-Vascular Implant Surveillance and Interventional Outcomes Coordinated Registry Network-Medicare-linked dataset, this study compared operative and long-term outcomes after CCAB and staged approaches.
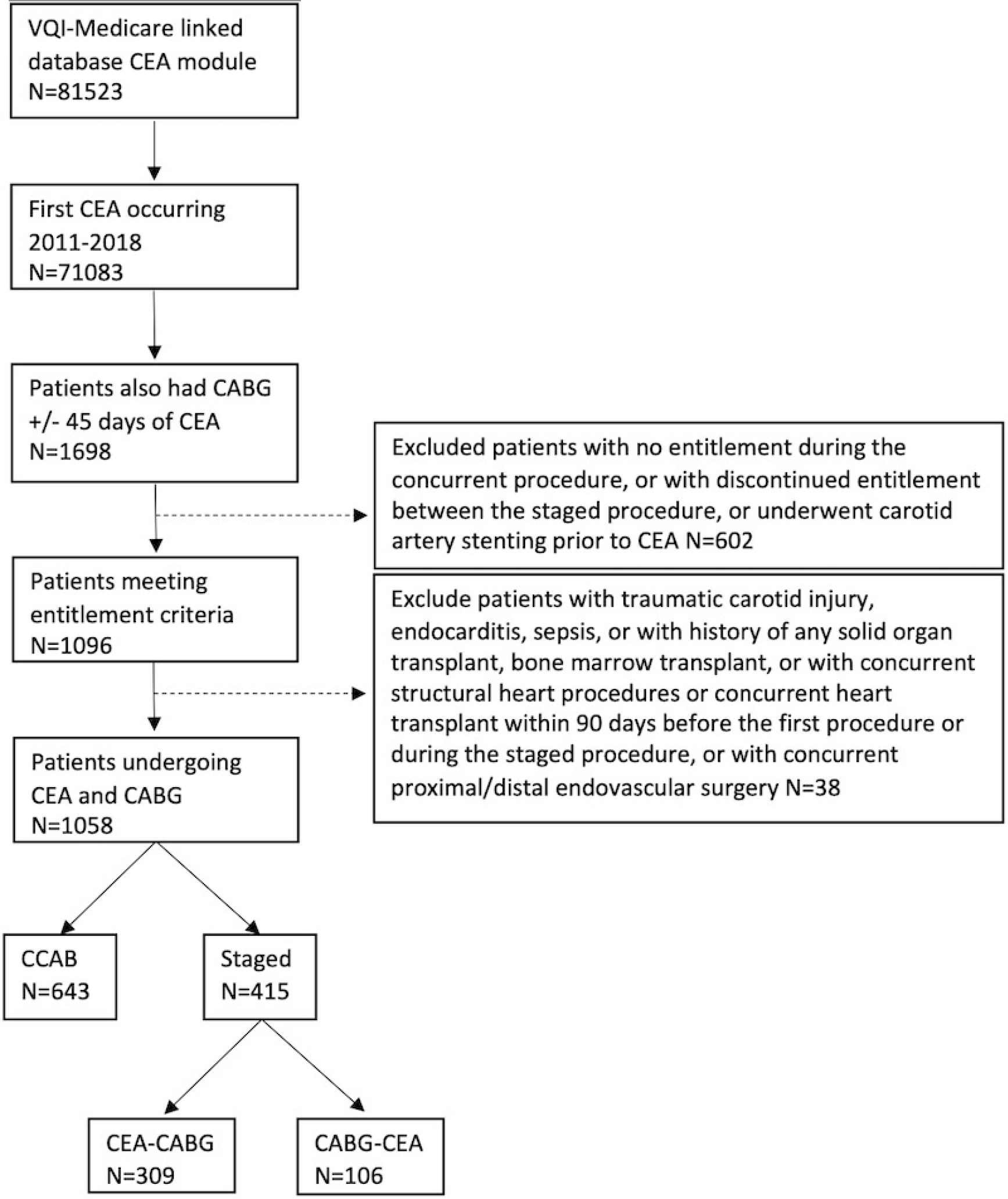
Methods: The Vascular Quality Initiative-Vascular Implant Surveillance and Interventional Outcomes Coordinated Registry Network dataset was used to identify CEAs from 2011 to 2018 with combined CABG or CABG within 45 days preceding or after CEA. Patients were stratified based on concurrent or staged approach. Primary outcomes were stroke, myocardial infarction (MI), all-cause mortality, stroke and death as composite (SD) and all as composite within 30 days from the last procedure as well as in the long term. Univariate analysis and risk-adjusted analysis using inverse propensity weighting were performed. Kaplan-Meier curves of stroke, MI, and death were created and compared.
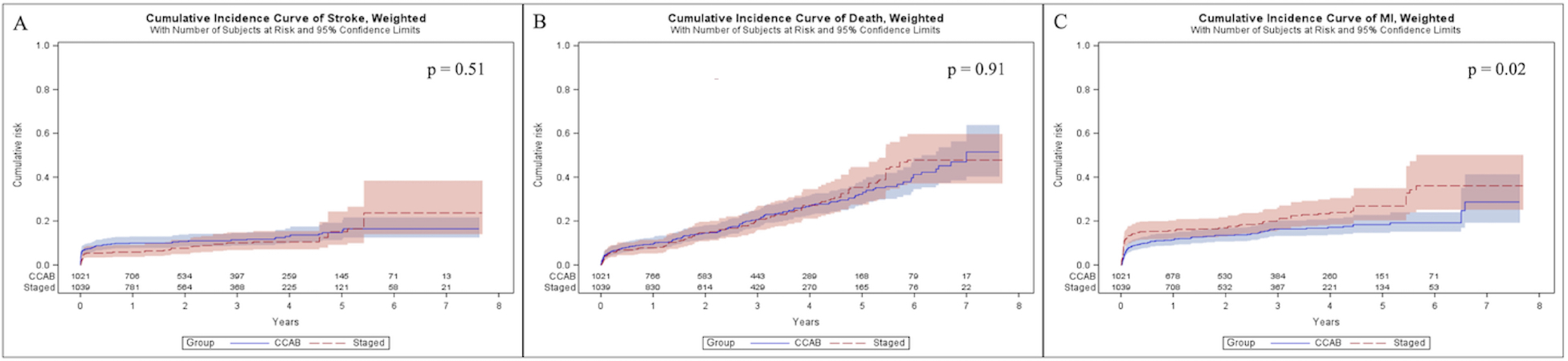
Results: There were 1058 patients included: 643 CCAB and 415 staged (309 CEA-CABG and 106 CABG-CEA). Compared with staged patients, those undergoing CCAB had a higher preoperative rate of congestive heart failure (24.8% vs 18.4%; P = .01) and decreased renal function (14.9% vs 8.5%; P < .01), as well as fewer prior neurological events (23.5% vs 31.4%; P < .01). Patients undergoing CCAB had similar weighted rate of 30-day stroke (4.6% vs 4.1%; P = .72), death (7.0% vs 5.0%; P = .32), and composite outcomes (stroke and death, 9.8% vs 8.5%; P = .56; stroke, death, and MI, 14.7% vs 17.4%; P = .31), but a lower weighted rate of MI (5.5% vs 11.5%; P < .01) vs the staged cohort. Long-term adjusted risks of stroke (hazard ratio [HR], 0.85; 95% confidence interval [CI], 0.54-1.36; P = .51) and mortality (HR, 1.02; 95% CI, 0.76-1.36; P=.91) were similar between groups, but higher risk of MI long-term was seen in those staged (HR, 1.49; 95% CI, 1.07-2.08; P = .02).
Conclusions: In patients undergoing CCAB or staged open revascularization for carotid stenosis and coronary artery disease, the staged approach had an increased risk of postoperative cardiac event, but the short- and long-term rates of stroke and mortality seem to be comparable. Adverse cardiovascular event risk is high between operations when staged and should be a consideration when selecting an approach. Although factors leading to staged sequencing performance need further clarity, CCAB seems to be safe and should be considered an equally reasonable option.
Keywords: Carotid endarterectomy; Carotid stenosis; Coronary artery bypass grafting; Coronary artery disease.
Copyright © 2023 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
The effect of combining coronary bypass with carotid endarterectomy in patients with unrevascularized severe coronary disease.J Vasc Surg. 2019 Sep;70(3):815-823. doi: 10.1016/j.jvs.2018.12.026. Epub 2019 Mar 6. J Vasc Surg. 2019. PMID: 30850293
-
Comparison of Trends and In-Hospital Outcomes of Concurrent Carotid Artery Revascularization and Coronary Artery Bypass Graft Surgery: The United States Experience 2004 to 2012.JACC Cardiovasc Interv. 2017 Feb 13;10(3):286-298. doi: 10.1016/j.jcin.2016.11.032. JACC Cardiovasc Interv. 2017. PMID: 28183469
-
The effect of clinical coronary disease severity on outcomes of carotid endarterectomy with and without combined coronary bypass.J Vasc Surg. 2020 Feb;71(2):546-552. doi: 10.1016/j.jvs.2019.03.074. Epub 2019 Aug 7. J Vasc Surg. 2020. PMID: 31401112
-
Systematic review and meta-analysis of the treatment strategies for coronary artery bypass graft patients with concomitant carotid artery atherosclerotic disease.J Vasc Surg. 2023 Oct;78(4):1083-1094.e8. doi: 10.1016/j.jvs.2023.04.043. Epub 2023 May 29. J Vasc Surg. 2023. PMID: 37257673
-
Synchronous versus Staged Carotid Endarterectomy and Coronary Artery Bypass Graft for Patients with Concomitant Severe Coronary and Carotid Artery Stenosis: A Systematic Review and Meta-analysis.Ann Vasc Surg. 2020 Feb;63:427-438.e1. doi: 10.1016/j.avsg.2019.09.007. Epub 2019 Oct 17. Ann Vasc Surg. 2020. PMID: 31629126
Cited by
-
Early and Long-Term Results of Simultaneous and Staged Revascularization of Coronary and Carotid Arteries.Pathophysiology. 2024 Apr 13;31(2):210-224. doi: 10.3390/pathophysiology31020017. Pathophysiology. 2024. PMID: 38651405 Free PMC article.
-
A Routine Coronary Angiography before Carotid Endarterectomy as an Example of Interdisciplinary Work: The Immediate Results of the Surgery.J Clin Med. 2024 Sep 17;13(18):5495. doi: 10.3390/jcm13185495. J Clin Med. 2024. PMID: 39336981 Free PMC article.
-
Management of Infective Endocarditis and Tibioperoneal Mycotic Aneurysm Following COVID-19 Infection.EJVES Vasc Forum. 2023 Sep 26;60:68-72. doi: 10.1016/j.ejvsvf.2023.09.005. eCollection 2023. EJVES Vasc Forum. 2023. PMID: 37881769 Free PMC article.
-
Early-Staged Carotid Artery Stenting Prior to Coronary Artery Bypass Grafting: Analysis of the Early and Mid-Term Results in Comparison with a Consecutive Cohort of Isolated Coronary Artery Surgery Patients.J Clin Med. 2024 Jan 15;13(2):480. doi: 10.3390/jcm13020480. J Clin Med. 2024. PMID: 38256614 Free PMC article.
-
Evaluating Carotid Plaque Stiffness with Ultrasound 2D Shear-Wave Elastography in Patients Undergoing Coronary Artery Bypass Grafting.Diagnostics (Basel). 2025 Jan 31;15(3):338. doi: 10.3390/diagnostics15030338. Diagnostics (Basel). 2025. PMID: 39941268 Free PMC article.
References
-
- Sharma V, Deo SV, Park SJ, Joyce LD. Meta-analysis of staged versus combined carotid endarterectomy and coronary artery bypass grafting. Ann Thorac Surg. 2014;97(1):102–109. - PubMed
-
- Taylor C, Walsh E, Stamm S. Synchronous CEA and CABG in asymptomatic carotid artery stenosis: A case study. J Vasc Nurs. 2019;37(3):194–198. - PubMed
-
- Naylor AR, Rantner B, Ancetti S, de Borst GJ, De Carlo M, Halliday A, et al. European society for vascular surgery (ESVS) 2023 Clinical practice guidelines on the management of atherosclerotic carotid and vertebral artery disease. Eur J Vasc Endovasc Surg. 2022. - PubMed
-
- Ricotta JJ, Aburahma A, Ascher E, Eskandari M, Faries P, Lal BK. Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease. J Vasc Surg. 2011;54(3):e1–31. - PubMed
-
- Naylor AR, Ricco JB, de Borst GJ, Debus S, de Haro J, Halliday A, et al. Editor’s Choice-Management of Atherosclerotic Carotid and Vertebral Artery Disease: 2017 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(1):3–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
