

Micropapillary and Solid Histologic Patterns in N1 and N2 Lymph Node Metastases Are Independent Factors of Poor Prognosis in Patients With Stages II to III Lung Adenocarcinoma
- PMID: 36681298
- PMCID: PMC10122702
- DOI: 10.1016/j.jtho.2023.01.002
Micropapillary and Solid Histologic Patterns in N1 and N2 Lymph Node Metastases Are Independent Factors of Poor Prognosis in Patients With Stages II to III Lung Adenocarcinoma
Abstract
Introduction: High-grade histologic patterns are associated with poor prognosis in patients with primary nonmucinous lung adenocarcinoma (ADC). We investigated whether the presence of micropapillary (MIP), solid (SOL), or both patterns in lymph node (LN) metastases has prognostic value.
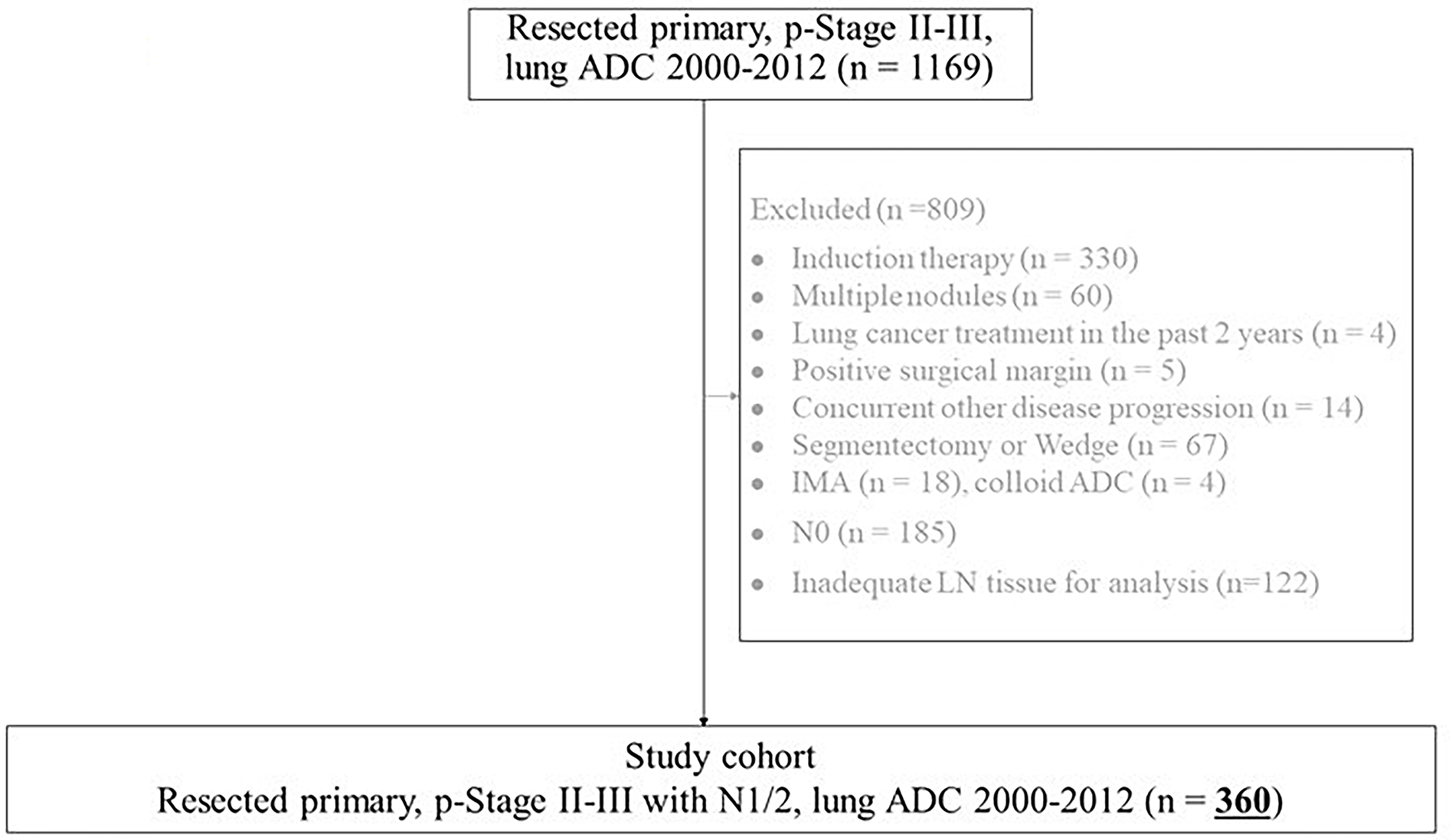
Methods: Patients who underwent lobectomy for pathologic stages II to III lung ADC with N1 or N2 LN metastases (N = 360; 2000-2012) were analyzed. We assessed overall survival (OS), lung cancer-specific cumulative incidence of death (LC-CID), and cumulative incidence of recurrence (CIR) between patients with and without MIP/SOL patterns in LN metastases. Multivariable Cox regression analysis was used to quantify the association between MIP/SOL patterns and outcomes.
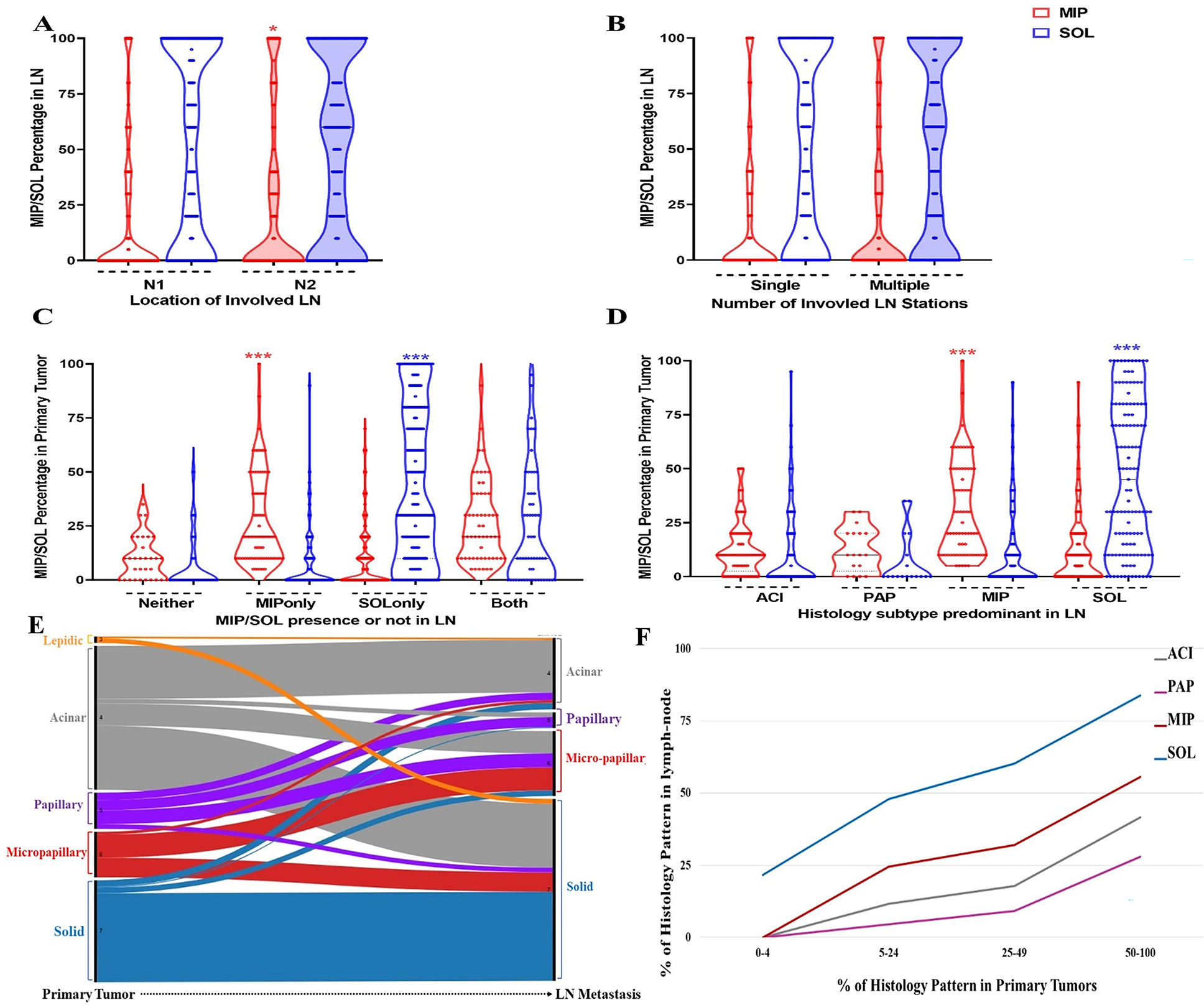
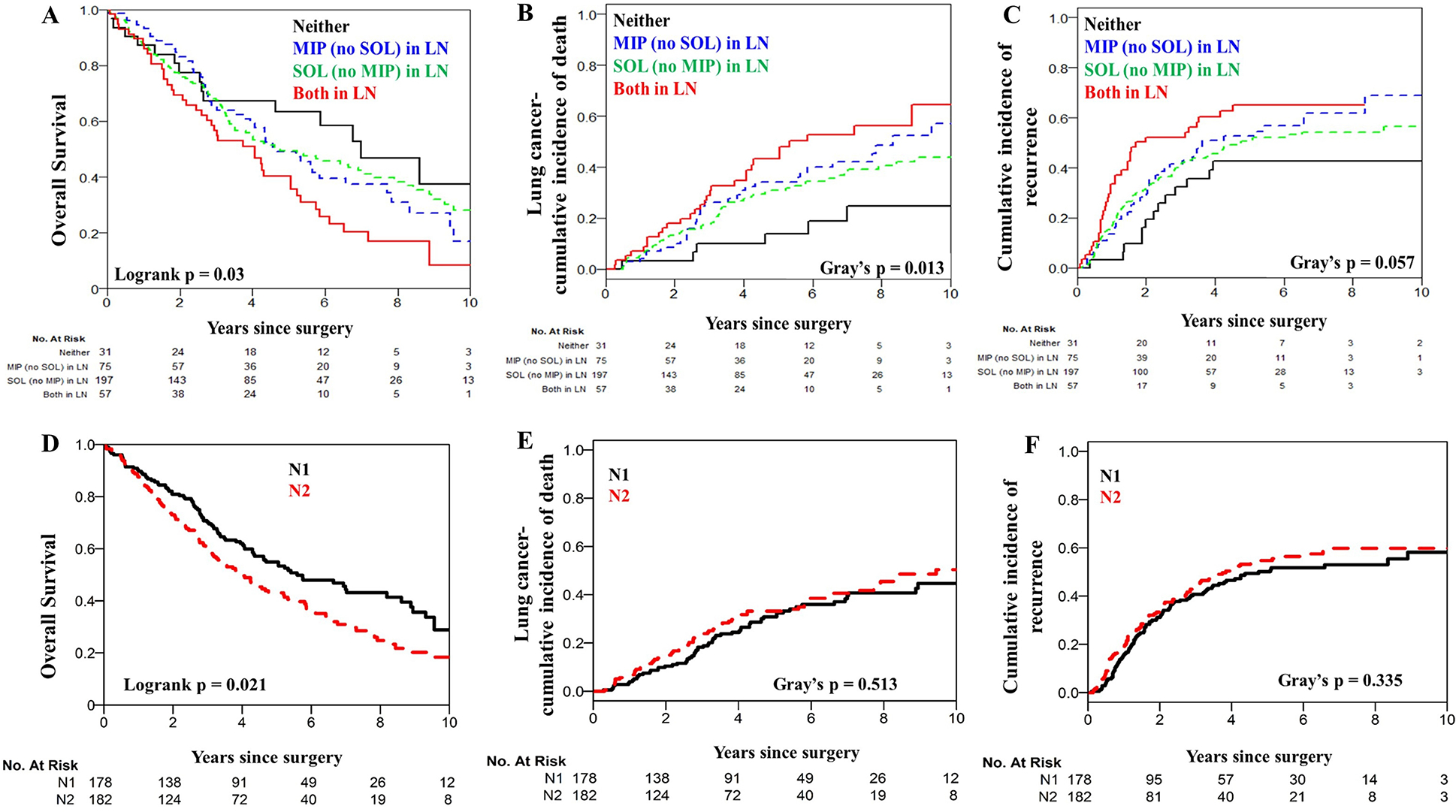
Results: MIP and SOL in LN metastases were associated with a higher incidence of smoking history (p = 0.004), tumor necrosis (p = 0.013), and spread of tumor through air spaces (p < 0.0001), a higher prevalence of MIP or SOL in the primary tumor (p < 0.0001), shorter OS (5-y OS, 40% [95% confidence interval or CI: 29%-56%] versus 63% [48%-83%] for no MIP/SOL in LNs, p = 0.03), higher LC-CID (5-y, 43% [29%-56%] versus 14% [4%-29%], p = 0.013), and higher CIR (5-y, 65% [50%-77%] versus 43% [25%-60%], p = 0.057). MIP and SOL in LN metastases were independently associated with poor outcomes: OS (hazard ratio [HR] = 1.81 [95% CI: 1.00-3.29], p = 0.05), LC-CID (HR = 3.10 [1.30-7.37], p = 0.01), and CIR (HR = 2.06 [1.09-3.90], p = 0.026).
Conclusions: MIP/SOL histologic patterns in N1 or N2 LN metastases are associated with worse outcomes in patients with stages II to III lung ADC. MIP/SOL histologic patterns in LN metastases can stratify patients with high-risk stages II to III lung ADC.
Keywords: Micropapillary adenocarcinoma; N classification; Nodal metastasis; Non–small cell lung cancer; Solid adenocarcinoma.
Copyright © 2023 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Memorial Sloan Kettering Cancer Center has licensed intellectual property related to mesothelin-targeted CARs and T-cell therapies to ATARA Biotherapeutics and has associated financial interests.
Figures
Comment in
-
Which Percentage of Micropapillary and Solid Histologic Patterns in Lymph Node Metastases Is Significantly Associated With Poor Outcomes?J Thorac Oncol. 2023 Jul;18(7):e75-e76. doi: 10.1016/j.jtho.2023.04.006. J Thorac Oncol. 2023. PMID: 37348998 No abstract available.
References
-
- Asamura H, Chansky K, Crowley J, et al. The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the N Descriptors in the Forthcoming 8th Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2015;10:1675–1684. 10.1097/jto.0000000000000678. - DOI - PubMed
-
- Yun JK, Lee GD, Choi S, et al. Comparison between lymph node station- and zone-based classification for the future revision of node descriptors proposed by the International Association for the Study of Lung Cancer in surgically resected patients with non-small-cell lung cancer. Eur J Cardiothorac Surg 2019;56:849–857. 10.1093/ejcts/ezz147. - DOI - PubMed
-
- Chiappetta M, Lococo F, Leuzzi G, et al. External validation of the N descriptor in the proposed tumour-node-metastasis subclassification for lung cancer: the crucial role of histological type, number of resected nodes and adjuvant therapy. Eur J Cardiothorac Surg 2020;58:1236–1244. 10.1093/ejcts/ezaa215. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
