

DNA damage triggers squamous metaplasia in human lung and mammary cells via mitotic checkpoints
- PMID: 36681661
- PMCID: PMC9867756
- DOI: 10.1038/s41420-023-01330-3
DNA damage triggers squamous metaplasia in human lung and mammary cells via mitotic checkpoints
Abstract
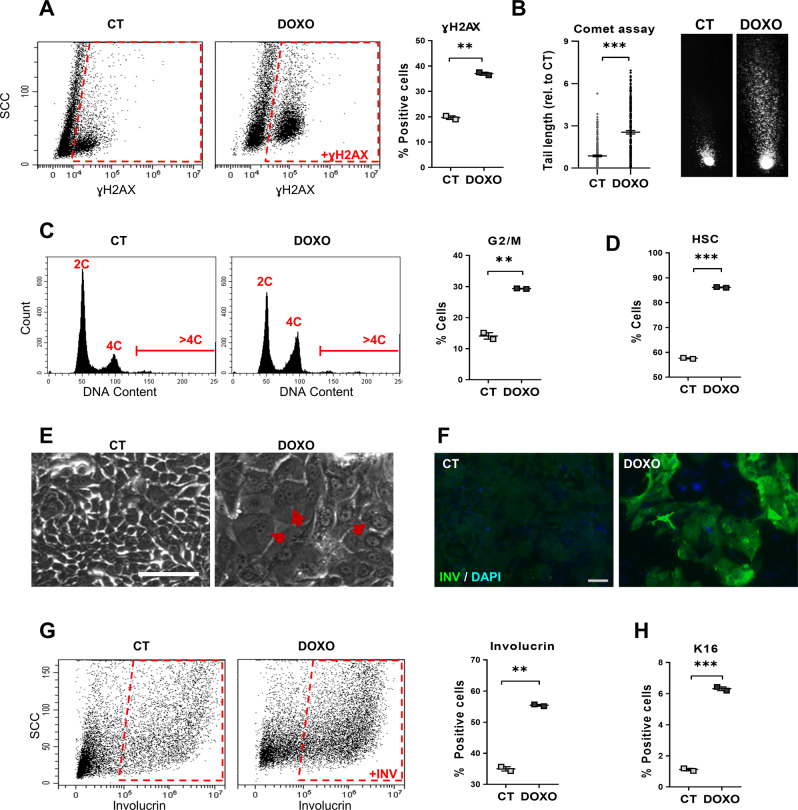
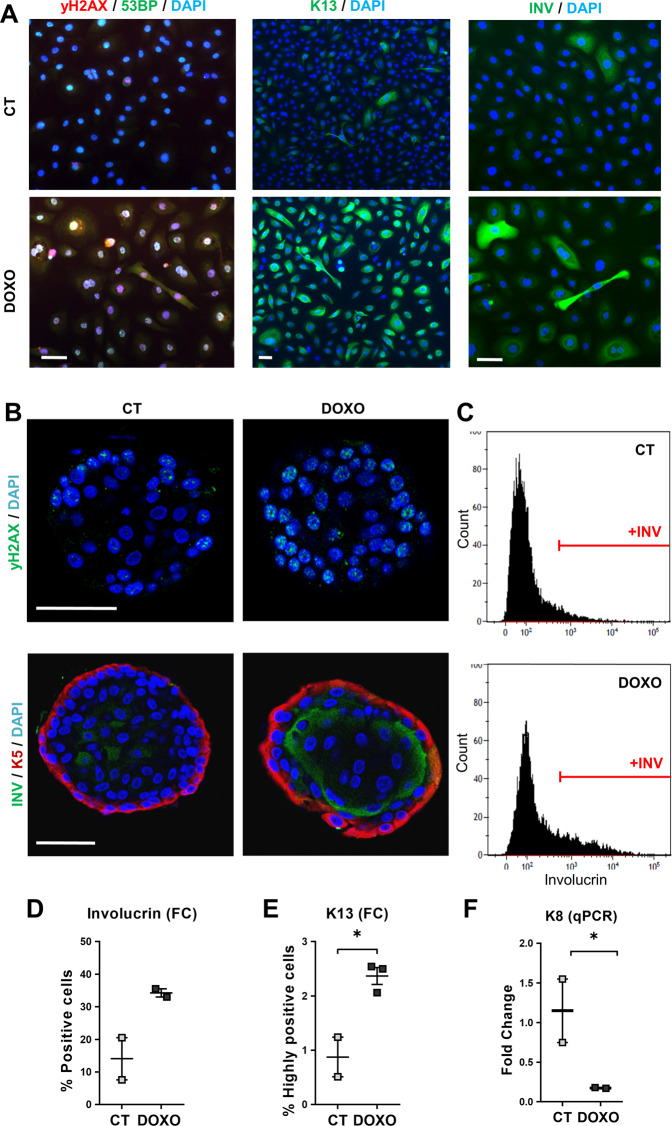
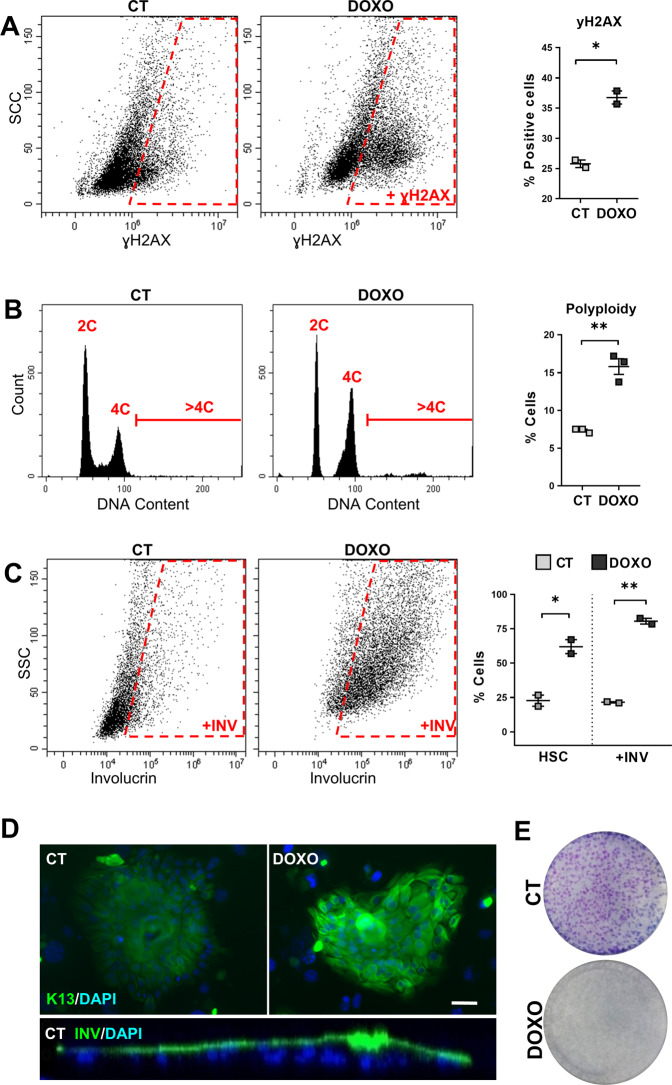
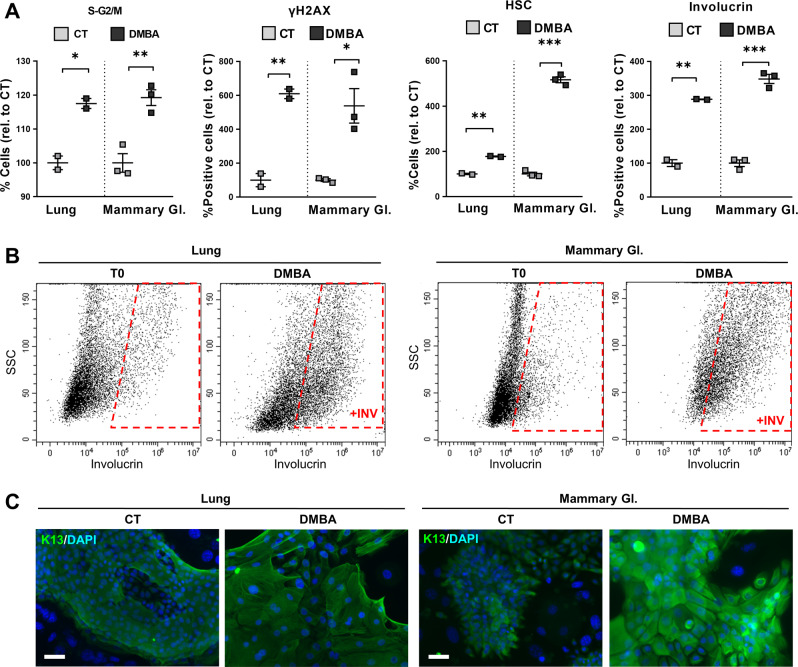
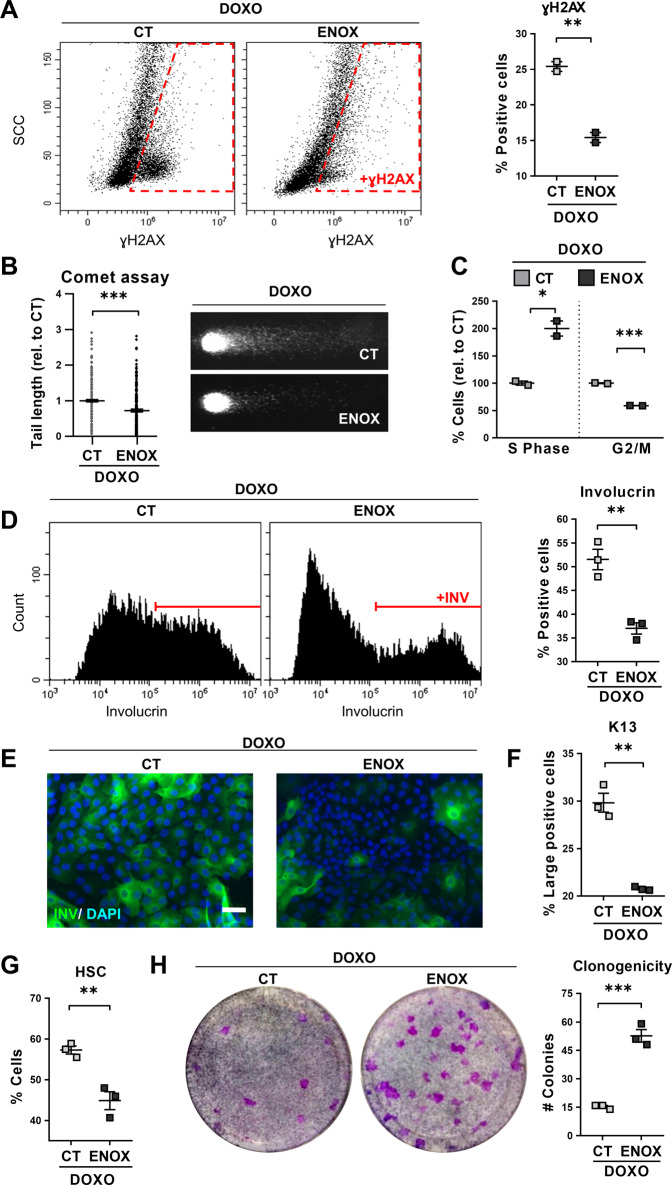
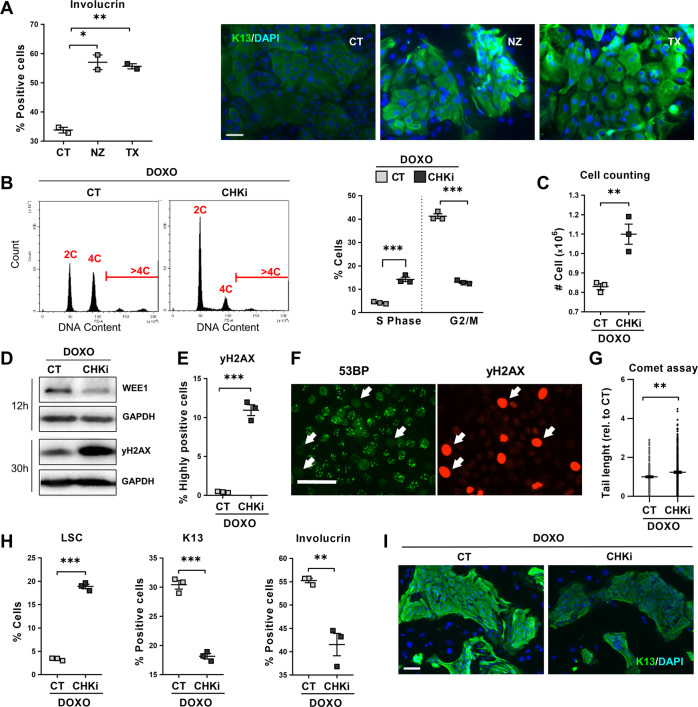
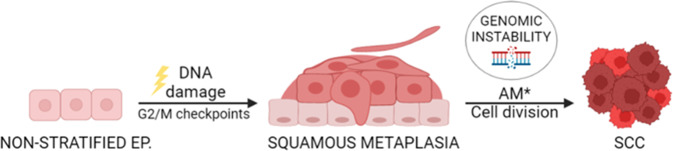
Epithelial transdifferentiation is frequent in tissue hyperplasia and contributes to disease in various degrees. Squamous metaplasia (SQM) precedes epidermoid lung cancer, an aggressive and frequent malignancy, but it is rare in the epithelium of the mammary gland. The mechanisms leading to SQM in the lung have been very poorly investigated. We have studied this issue on human freshly isolated cells and organoids. Here we show that human lung or mammary cells strikingly undergo SQM with polyploidisation when they are exposed to genotoxic or mitotic drugs, such as Doxorubicin or the cigarette carcinogen DMBA, Nocodazole, Taxol or inhibitors of Aurora-B kinase or Polo-like kinase. To note, the epidermoid response was attenuated when DNA repair was enhanced by Enoxacin or when mitotic checkpoints where abrogated by inhibition of Chk1 and Chk2. The results show that DNA damage has the potential to drive SQM via mitotic checkpoints, thus providing novel molecular candidate targets to tackle lung SCC. Our findings might also explain why SCC is frequent in the lung, but not in the mammary gland and why chemotherapy often causes complicating skin toxicity.
© 2023. The Author(s).
Conflict of interest statement
HC is an inventor of patents related to organoid research, His full disclosure:
Figures
Similar articles
-
Response of head and neck epithelial cells to a DNA damage-differentiation checkpoint involving polyploidization.Head Neck. 2018 Nov;40(11):2487-2497. doi: 10.1002/hed.25376. Epub 2018 Oct 12. Head Neck. 2018. PMID: 30311985
-
Inhibitory effects of retinoids on development of squamous metaplasia in rat mammary epithelial organoids cultured in Matrigel.Cancer Lett. 1996 Dec 20;110(1-2):217-23. doi: 10.1016/s0304-3835(96)04514-4. Cancer Lett. 1996. PMID: 9018105
-
Context-dependent cell cycle checkpoint abrogation by a novel kinase inhibitor.PLoS One. 2010 Oct 18;5(10):e13123. doi: 10.1371/journal.pone.0013123. PLoS One. 2010. PMID: 20976184 Free PMC article.
-
Structure meets function--centrosomes, genome maintenance and the DNA damage response.Exp Cell Res. 2006 Aug 15;312(14):2633-40. doi: 10.1016/j.yexcr.2006.06.008. Epub 2006 Jun 20. Exp Cell Res. 2006. PMID: 16854412 Review.
-
Carcinoma of the lung in Okinawa, Japan: with special reference to squamous cell carcinoma and squamous metaplasia.Pathol Int. 1997 Oct;47(10):659-72. doi: 10.1111/j.1440-1827.1997.tb04439.x. Pathol Int. 1997. PMID: 9361099 Review.
Cited by
-
Natural compound chaetocin induced DNA damage and apoptosis through reactive oxygen species-dependent pathways in A549 lung cancer cells and in vitro evaluations.IET Nanobiotechnol. 2023 Jul;17(5):465-475. doi: 10.1049/nbt2.12144. Epub 2023 Jul 7. IET Nanobiotechnol. 2023. PMID: 37417682 Free PMC article.
-
Sumo-regulatory SENP2 controls the homeostatic squamous mitosis-differentiation checkpoint.Cell Death Dis. 2024 Aug 16;15(8):596. doi: 10.1038/s41419-024-06969-z. Cell Death Dis. 2024. PMID: 39152119 Free PMC article.
-
DNA damage signalling histone H2AX is required for tumour growth.Cell Death Discov. 2024 Feb 24;10(1):99. doi: 10.1038/s41420-024-01869-9. Cell Death Discov. 2024. PMID: 38402225 Free PMC article.
-
The potential of the South African plant Tulbaghia Violacea Harv for the treatment of triple negative breast cancer.Sci Rep. 2025 Feb 17;15(1):5737. doi: 10.1038/s41598-025-88417-2. Sci Rep. 2025. PMID: 39962120 Free PMC article.
-
Traffic light at DSB-transit regulation between gene transcription and DNA repair.FEBS Lett. 2025 Jan;599(2):177-189. doi: 10.1002/1873-3468.15024. Epub 2024 Sep 27. FEBS Lett. 2025. PMID: 39333024 Free PMC article. Review.
References
-
- Boni R, Schuster C, Nehrhoff B, Burg G. Epidemiology of skin cancer. Neuro Endocrinol Lett. 2002;23(Suppl 2):48–51. - PubMed
-
- World Cancer Research Fund International, 2022. http://www.wcrf.org.
Grants and funding
- (ISCIII)-FEDER, PI17/03107/Ministry of Economy and Competitiveness | Instituto de Salud Carlos III (Institute of Health Carlos III)
- (ISCIII)-FEDER, PI20/00880/Ministry of Economy and Competitiveness | Instituto de Salud Carlos III (Institute of Health Carlos III)
- 024.003.001/Ministerie van Onderwijs, Cultuur en Wetenschap (Ministry of Education, Culture and Science, Netherlands)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
