

Dynamic predictions of postoperative complications from explainable, uncertainty-aware, and multi-task deep neural networks
- PMID: 36681755
- PMCID: PMC9867692
- DOI: 10.1038/s41598-023-27418-5
Dynamic predictions of postoperative complications from explainable, uncertainty-aware, and multi-task deep neural networks
Abstract
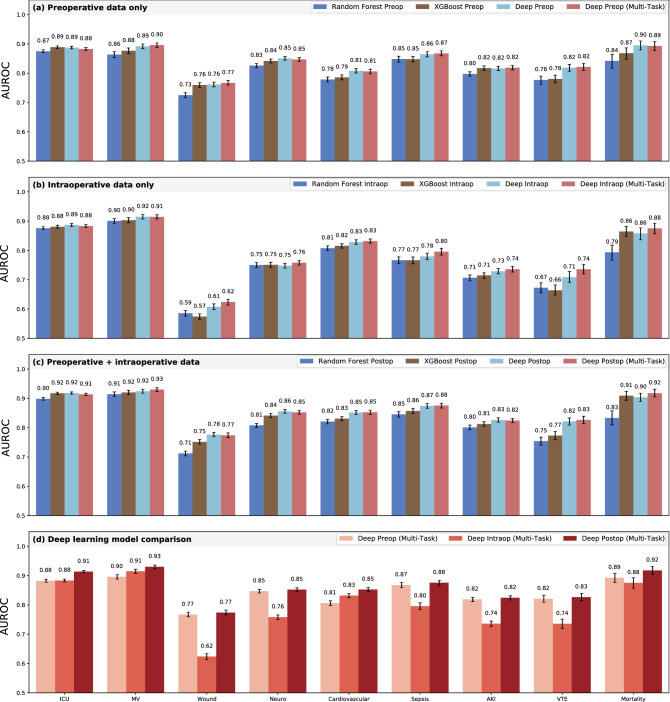
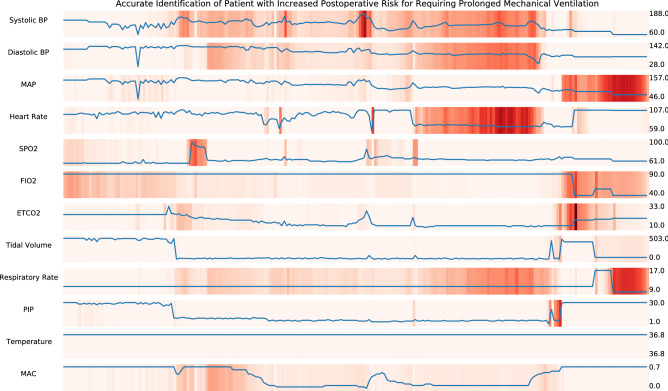
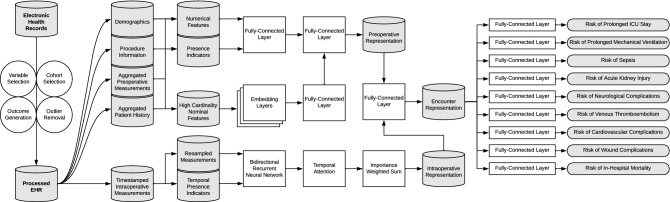
Accurate prediction of postoperative complications can inform shared decisions regarding prognosis, preoperative risk-reduction, and postoperative resource use. We hypothesized that multi-task deep learning models would outperform conventional machine learning models in predicting postoperative complications, and that integrating high-resolution intraoperative physiological time series would result in more granular and personalized health representations that would improve prognostication compared to preoperative predictions. In a longitudinal cohort study of 56,242 patients undergoing 67,481 inpatient surgical procedures at a university medical center, we compared deep learning models with random forests and XGBoost for predicting nine common postoperative complications using preoperative, intraoperative, and perioperative patient data. Our study indicated several significant results across experimental settings that suggest the utility of deep learning for capturing more precise representations of patient health for augmented surgical decision support. Multi-task learning improved efficiency by reducing computational resources without compromising predictive performance. Integrated gradients interpretability mechanisms identified potentially modifiable risk factors for each complication. Monte Carlo dropout methods provided a quantitative measure of prediction uncertainty that has the potential to enhance clinical trust. Multi-task learning, interpretability mechanisms, and uncertainty metrics demonstrated potential to facilitate effective clinical implementation.
© 2023. The Author(s).
Conflict of interest statement
The authors have no competing interests as defined by Nature Research, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
