

Therapeutic beta-lactam dosages and broad-spectrum antibiotics are associated with reductions in microbial richness and diversity in persons with cystic fibrosis
- PMID: 36681756
- PMCID: PMC9867719
- DOI: 10.1038/s41598-023-27628-x
Therapeutic beta-lactam dosages and broad-spectrum antibiotics are associated with reductions in microbial richness and diversity in persons with cystic fibrosis
Abstract
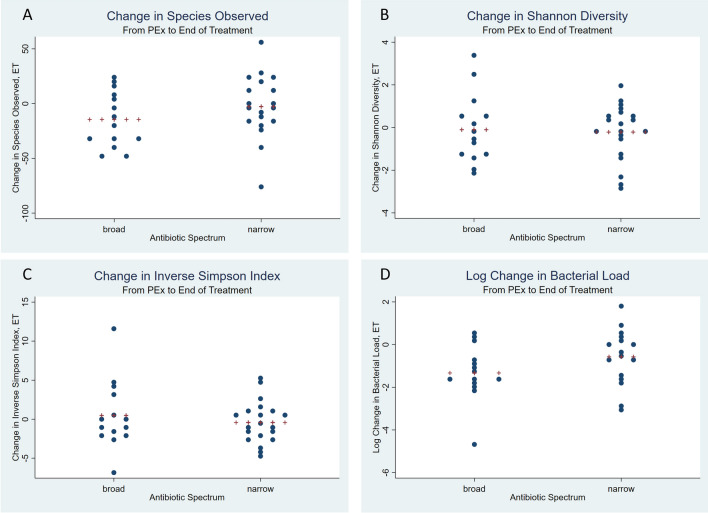
Persons with cystic fibrosis (PwCF) suffer from pulmonary exacerbations (PEx) related in part to lung infection. While higher microbial diversity is associated with higher lung function, the data on the impact of short-term antibiotics on changes in microbial diversity is conflicting. Further, Prevotella secretes beta-lactamases, which may influence recovery of lung function. We hypothesize that sub-therapeutic and broad spectrum antibiotic exposure leads to decreasing microbial diversity. Our secondary aim was to evaluate the concerted association of beta-lactam pharmacokinetics (PK), antibiotic spectrum, microbial diversity, and antibiotic resistance on lung function recovery using a pathway analysis. This was a retrospective observational study of persons with CF treated with IV antibiotics for PEx between 2016 and 2020 at Children's National Hospital; respiratory samples and clinical information were collected at hospital admission for PEx (E), end of antibiotic treatment (T), and follow-up (F). Metagenomic sequencing was performed; PathoScope 2.0 and AmrPlusPlus were used for taxonomic assignment of sequences to bacteria and antibiotic resistance genes (ARGs). M/W Pharm was used for PK modeling. Comparison of categorical and continuous variables and pathway analysis were performed in STATA. Twenty-two PwCF experienced 43 PEx. The study cohort had a mean age of 14.6 years. Only 12/43 beta-lactam courses had therapeutic PK, and 18/43 were broad spectrum. A larger decrease in richness between E and T was seen in the therapeutic PK group (sufficient - 20.1 vs. insufficient - 1.59, p = 0.025) and those receiving broad spectrum antibiotics (broad - 14.5 vs. narrow - 2.8, p = 0.030). We did not detect differences in the increase in percent predicted forced expiratory volume in one second (ppFEV1) at end of treatment compared to PEx based on beta-lactam PK (sufficient 13.6% vs. insufficient 15.1%) or antibiotic spectrum (broad 11.5% vs. narrow 16.6%). While both therapeutic beta-lactam PK and broad-spectrum antibiotics decreased richness between PEx and the end of treatment, we did not detect longstanding changes in alpha diversity or an association with superior recovery of lung function compared with subtherapeutic PK and narrow spectrum antimicrobials.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Importance of beta-lactam pharmacokinetics and pharmacodynamics on the recovery of microbial diversity in the airway of persons with cystic fibrosis.J Investig Med. 2021 Oct;69(7):1350-1359. doi: 10.1136/jim-2021-001824. Epub 2021 May 21. J Investig Med. 2021. PMID: 34021052 Free PMC article.
-
Changes in microbiome diversity following beta-lactam antibiotic treatment are associated with therapeutic versus subtherapeutic antibiotic exposure in cystic fibrosis.Sci Rep. 2019 Feb 22;9(1):2534. doi: 10.1038/s41598-019-38984-y. Sci Rep. 2019. PMID: 30796252 Free PMC article.
-
Association Between Number of Intravenous Antipseudomonal Antibiotics and Clinical Outcomes of Pediatric Cystic Fibrosis Pulmonary Exacerbations.Clin Infect Dis. 2021 Nov 2;73(9):1589-1596. doi: 10.1093/cid/ciab525. Clin Infect Dis. 2021. PMID: 34100912 Free PMC article.
-
Clinical features associated with pulmonary exacerbation diagnosis in infants and young children with cystic fibrosis.Pediatr Pulmonol. 2024 Apr;59(4):874-879. doi: 10.1002/ppul.26838. Epub 2023 Dec 22. Pediatr Pulmonol. 2024. PMID: 38131505 Review.
-
Pseudomonas aeruginosa chromosomal beta-lactamase in patients with cystic fibrosis and chronic lung infection. Mechanism of antibiotic resistance and target of the humoral immune response.APMIS Suppl. 2003;(116):1-47. APMIS Suppl. 2003. PMID: 14692154 Review.
Cited by
-
Current Trends in Antibiotic Therapy and Resistance: A Comparative Study of Various Spectrums.Cureus. 2025 Apr 9;17(4):e81956. doi: 10.7759/cureus.81956. eCollection 2025 Apr. Cureus. 2025. PMID: 40351959 Free PMC article.
-
Adjunctive phage therapy improves antibiotic treatment of ventilator-associated-pneumonia with Pseudomonas aeruginosa.Nat Commun. 2025 May 15;16(1):4500. doi: 10.1038/s41467-025-59806-y. Nat Commun. 2025. PMID: 40368965 Free PMC article.
-
Effects of Therapeutic Antibiotic Exposure on the Oropharyngeal and Fecal Microbiota in Infants With Cystic Fibrosis.Pediatr Pulmonol. 2025 Mar;60(3):e71024. doi: 10.1002/ppul.71024. Pediatr Pulmonol. 2025. PMID: 40042126 Free PMC article.
References
-
- Marshall, B. C. Cystic Fibrosis Foundation Patient Registry: 2020 Annual Data Report. https://www.cff.org/sites/default/files/2021-11/Patient-Registry-Annual-... (2021).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
