

Health Expectations and Quality of Life After Acute Respiratory Failure: A Multicenter Prospective Cohort Study
- PMID: 36682611
- PMCID: PMC10331625
- DOI: 10.1016/j.chest.2023.01.016
Health Expectations and Quality of Life After Acute Respiratory Failure: A Multicenter Prospective Cohort Study
Abstract
Background: Patients often have high expectations for recovery after critical illness, but the impact of these expectations on subsequent quality of life (QoL) after serious illnesses has not been evaluated empirically.
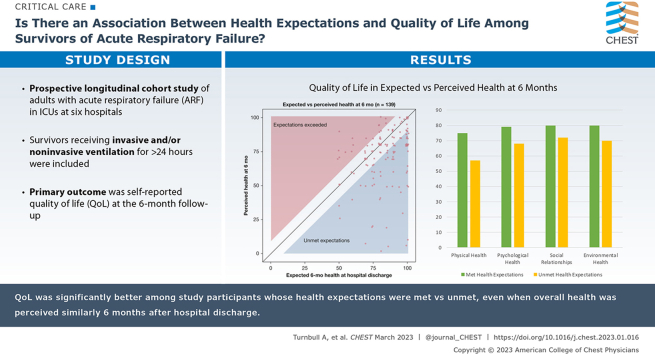
Research question: Among adult survivors of acute respiratory failure (ARF), are met vs unmet expectations for health associated with self-reported QoL 6 months after discharge?
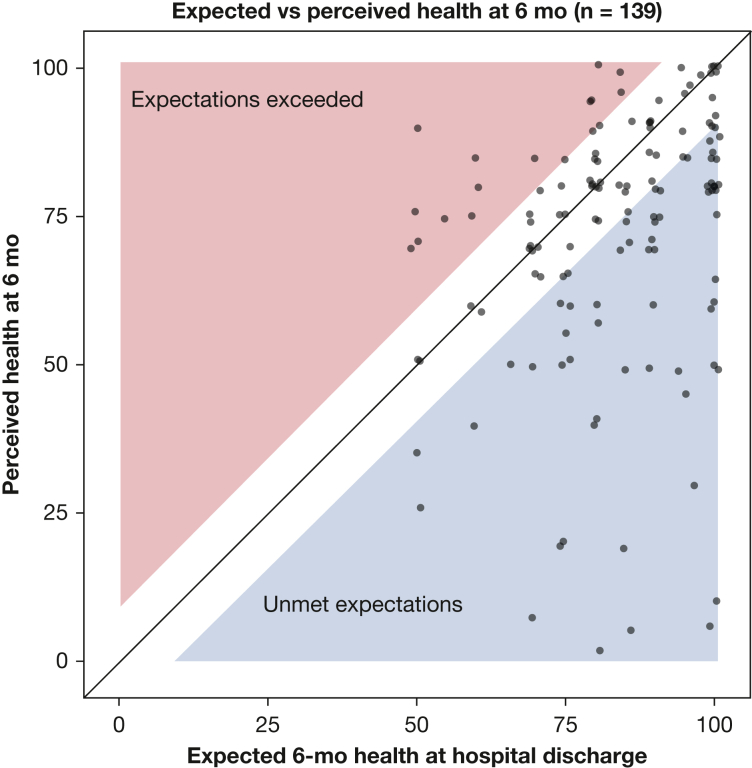
Study design and methods: This was a prospective longitudinal cohort study enrolling consecutive adult patients with ARF managed in ICUs at five academic medical centers. At hospital discharge, we evaluated participants' expected health 6 months in the future via a visual analog scale (VAS; range, 0-100), with higher scores representing better expected health. At 6-month follow-up, perceived health was assessed using the EQ-5D VAS, and QoL was assessed using the World Health Organization Quality of Life Brief Version (WHOQOL-BREF) instrument. Participants' health expectations were categorized as having been met when perceived health at 6 months was no more than eight points lower than their expectation at study enrollment. The primary analysis compared WHOQOL-BREF domain scores (range, 0-100) at 6 months after discharge in patients with met vs unmet health expectations using the nonparametric Mann-Whitney U test. Secondary analysis modeled WHOQOL-BREF domain scores using multivariate regression, and sensitivity analyses assessed QoL using EQ-5D-5L index values.
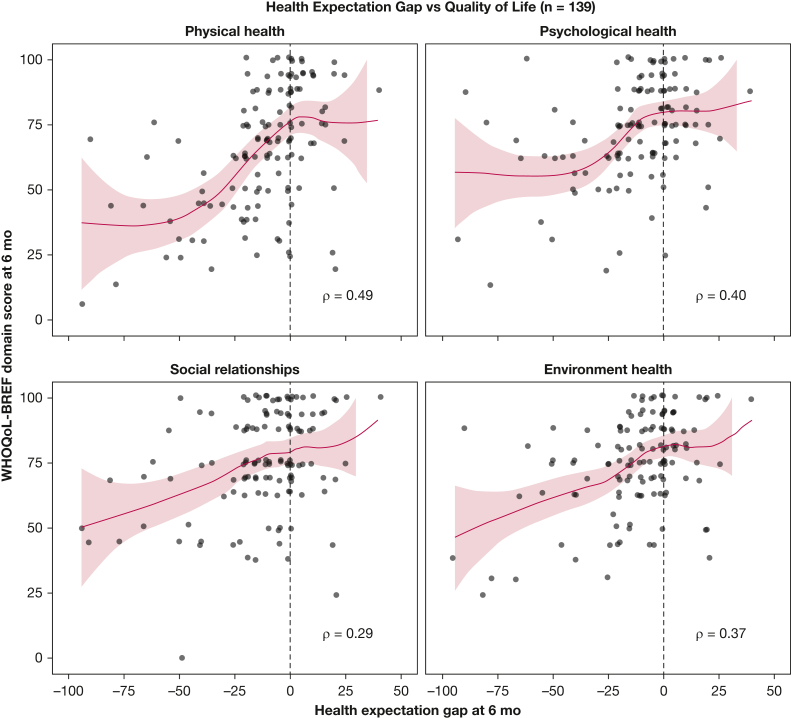
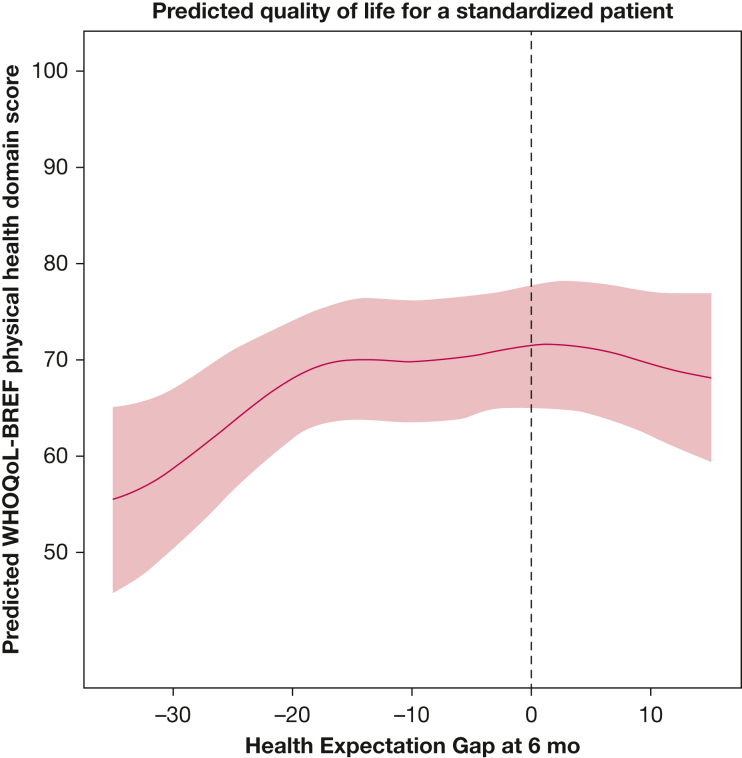
Results: In the primary analysis, QoL was significantly better among participants with met vs unmet health expectations across all domains of the WHOQOL-BREF: physical health (estimated difference in scores: median, 19 [interquartile range (IQR), 12-15]; P < .001), psychological health (median, 12 [IQR, 6-18]; P < .001), social relationships (median, 6 [IQR, 0-13]; P = .02), and environmental health (median, 12 [IQR, 6-13]; P < .001). In multivariate regression, the difference between expected and perceived health remained associated significantly with the physical health domain score.
Interpretation: Fulfillment of health expectations is associated with better QoL after ARF, suggesting a mechanism underpinning successful ICU recovery programs that incorporate normalization and expectation management.
Keywords: critical care outcomes; functional status; quality of life; respiratory distress syndrome; survivorship.
Copyright © 2023 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Rubenfeld G.D., Caldwell E., Peabody E., et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685–1693. - PubMed
-
- Zambon M., Vincent J.L. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest. 2008;133(5):1120–1127. - PubMed
-
- Phua J., Badia J.R., Adhikari N.K.J., et al. Has mortality from acute respiratory distress syndrome decreased over time? A systematic review. Am J Respir Crit Care Med. 2009;179(3):220–227. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
