

Guidelines for the Diagnosis and Treatment of Pediatric Familial Hypercholesterolemia 2022
- PMID: 36682777
- PMCID: PMC10164603
- DOI: 10.5551/jat.CR006
Guidelines for the Diagnosis and Treatment of Pediatric Familial Hypercholesterolemia 2022
Abstract
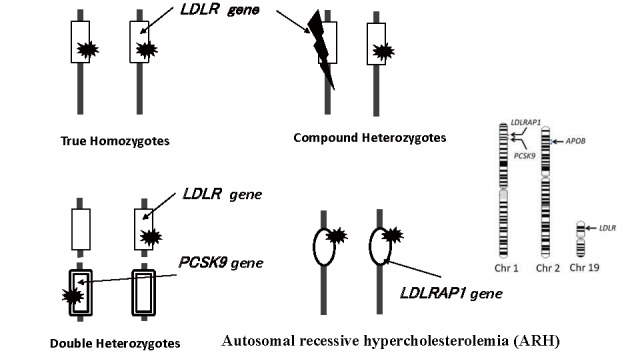
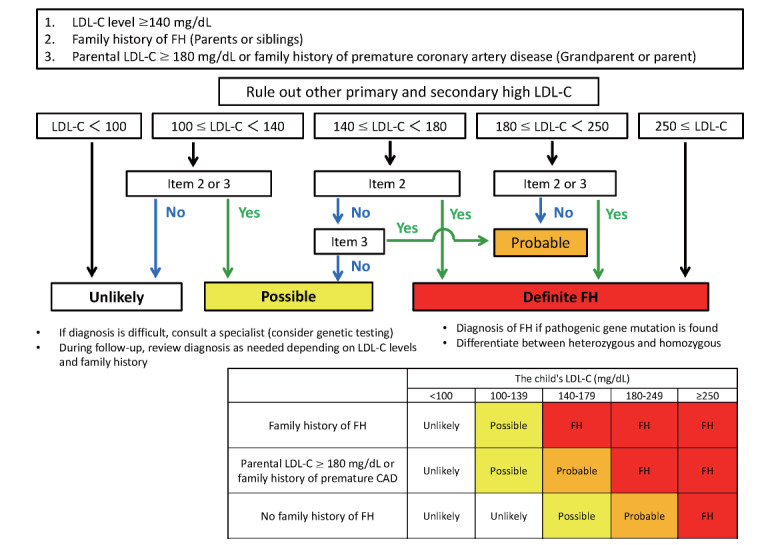
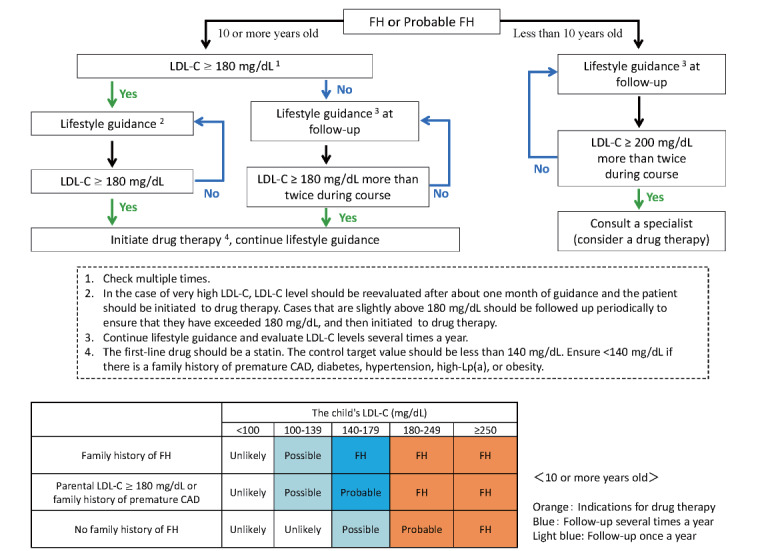
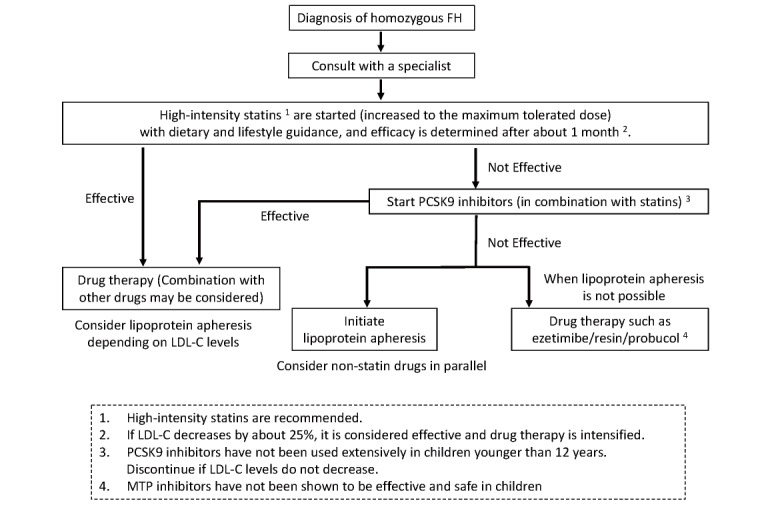
As atherosclerosis begins in childhood, early diagnosis and treatment of familial hypercholesterolemia (FH) is considered necessary. The basic diagnosis of pediatric FH (under 15 years of age) is based on hyper-low-density lipoprotein (LDL) cholesterolemia and a family history of FH; however, in this guideline, to reduce overlooked cases, "probable FH" was established. Once diagnosed with FH or probable FH, efforts should be made to promptly provide lifestyle guidance, including diet. It is also important to conduct an intrafamilial survey, to identify family members with the same condition. If the level of LDL-C remains above 180 mg/dL, drug therapy should be considered at the age of 10. The first-line drug should be statin. Evaluation of atherosclerosis should be started using non-invasive techniques, such as ultrasound. The management target level is an LDL-C level of less than 140 mg/dL. If a homozygous FH is suspected, consult a specialist and determine the response to pharmacotherapy with evaluating atherosclerosis. If the response is inadequate, initiate lipoprotein apheresis as soon as possible.
Keywords: Diagnostic criteria; Familial Hypercholesterolemia; Heterozygote; Homozygote; Lifestyle; Low-density lipoprotein apheresis; Pediatric; Pharmacological therapy; Statins; Treatment guidelines.
Conflict of interest statement
Figures
References
-
- Li S, Chen W, Srinivasan SR, Bond MG, Tang R, Urbina EM, Berenson GS: Childhood cardiovascular risk factors and carotid vascular changes in adulthood: the Bogalusa Heart Study. Jama, 2003; 290: 2271-2276 - PubMed
-
- Natural history of aortic and coronary atherosclerotic lesions in youth. Findings from the PDAY Study. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. Arterioscler Thromb, 1993; 13: 1291-1298 - PubMed
-
- Mabuchi H, Nohara A, Noguchi T, Kobayashi J, Kawashiri MA, Tada H, Nakanishi C, Mori M, Yamagishi M, Inazu A, Koizumi J: Molecular genetic epidemiology of homozygous familial hypercholesterolemia in the Hokuriku district of Japan. Atherosclerosis, 2011; 214: 404-407 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous