

A nationwide population-based study on the clinical and economic burden of anastomotic leakage in colorectal surgery
- PMID: 36683099
- PMCID: PMC9868041
- DOI: 10.1007/s00423-023-02809-4
A nationwide population-based study on the clinical and economic burden of anastomotic leakage in colorectal surgery
Abstract
Aim: Anastomotic leakage (AL) is one of the most dreaded complications in colorectal surgery. In 2013, the International Classification of Diseases code K91.83 for AL was introduced in Germany, allowing nationwide analysis of AL rates and associated parameters. The aim of this population-based study was to investigate the current incidence, risk factors, mortality, clinical management, and associated costs of AL in colorectal surgery.
Methods: A data query was performed based on diagnosis-related group data of all hospital cases of inpatients undergoing colon or sphincter-preserving rectal resections between 2013 and 2018 in Germany.
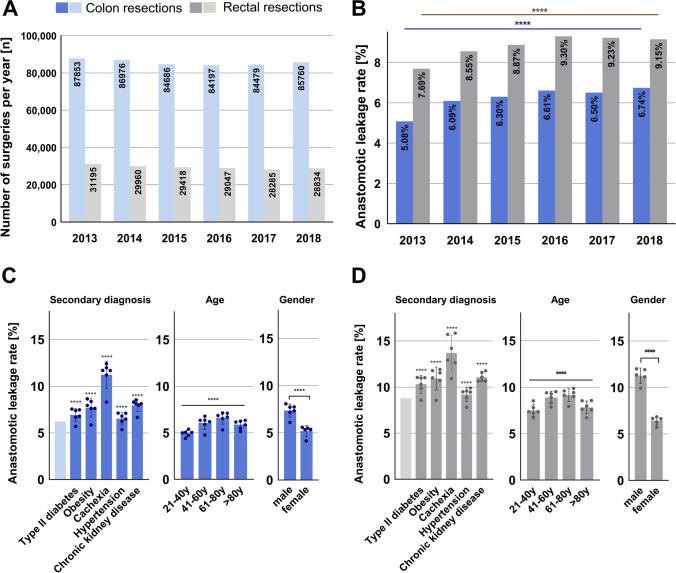
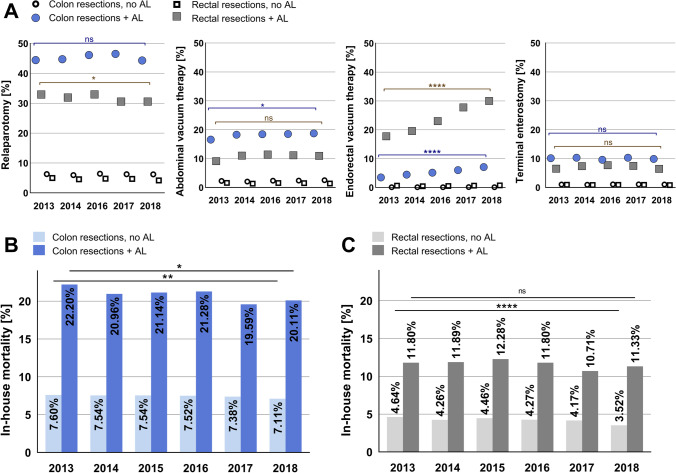
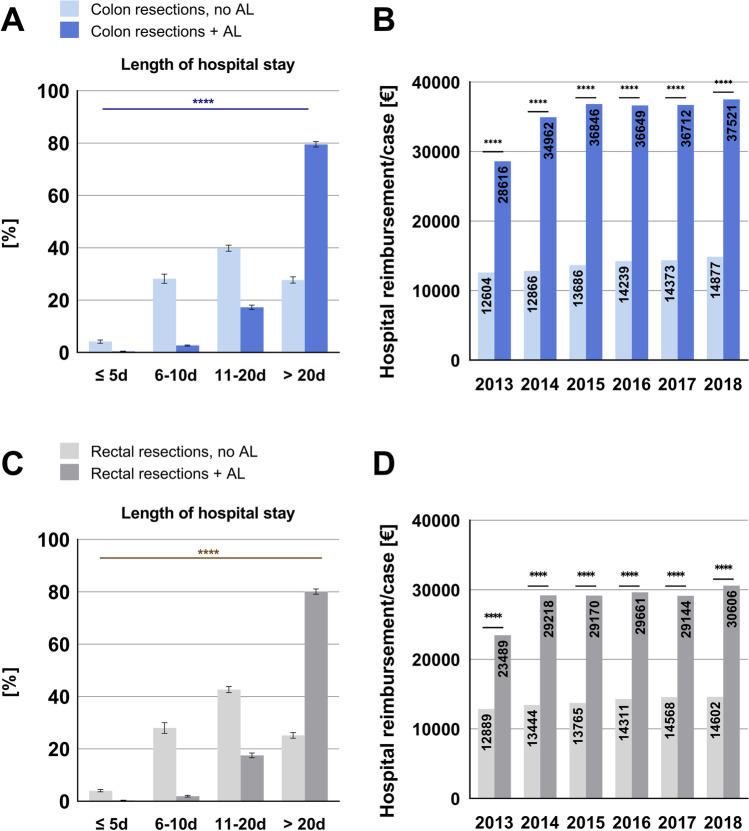
Results: A total number of 690,690 inpatient cases were included in this study. AL rates were 6.7% for colon resections and 9.2% for rectal resections in 2018. Regarding the treatment of AL, the application of endoluminal vacuum therapy increased during the studied period, while rates of relaparotomy, abdominal vacuum therapy, and terminal enterostomy remained stable. AL was associated with significantly increased in-house mortality (7.11% vs. 20.11% for colon resections and 3.52% vs. 11.33% for rectal resections in 2018) and higher socioeconomic costs (mean hospital reimbursement volume per case: 14,877€ (no AL) vs. 37,521€ (AL) for colon resections and 14,602€ (no AL) vs. 30,606€ (AL) for rectal resections in 2018).
Conclusions: During the studied time period, AL rates did not decrease, and associated mortality remained at a high level. Our study provides updated population-based data on the clinical and economic burden of AL in Germany. Focused research in the field of AL is still urgently necessary to develop targeted strategies to prevent AL, improve patient care, and decrease socioeconomic costs.
Keywords: Anastomotic leakage; Colorectal surgery; Postoperative complications.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ammann EM, Goldstein LJ, Nagle D, Wei D, Johnston SS. A dual-perspective analysis of the hospital and payer-borne burdens of selected in-hospital surgical complications in low anterior resection for colorectal cancer. Hosp Pract (1995) 2019;47(2):80–7. doi: 10.1080/21548331.2019.1568718. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
