

The Gut Microbiome Dynamically Associates with Host Glucose Metabolism throughout Pregnancy: Longitudinal Findings from a Matched Case-Control Study of Gestational Diabetes Mellitus
- PMID: 36683149
- PMCID: PMC10074094
- DOI: 10.1002/advs.202205289
The Gut Microbiome Dynamically Associates with Host Glucose Metabolism throughout Pregnancy: Longitudinal Findings from a Matched Case-Control Study of Gestational Diabetes Mellitus
Abstract
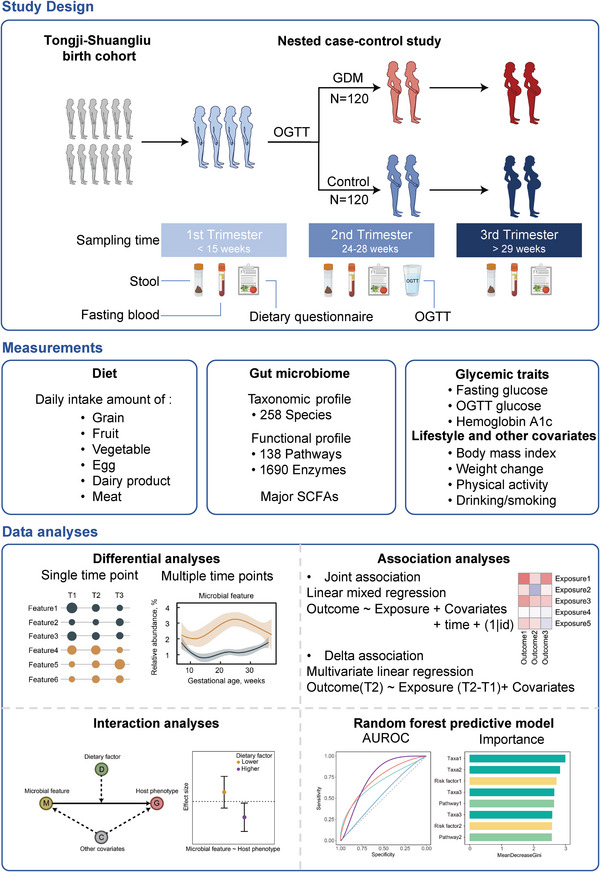
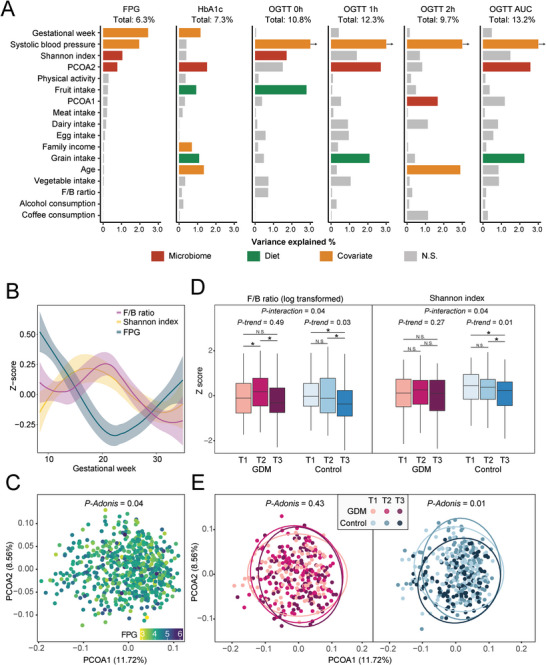
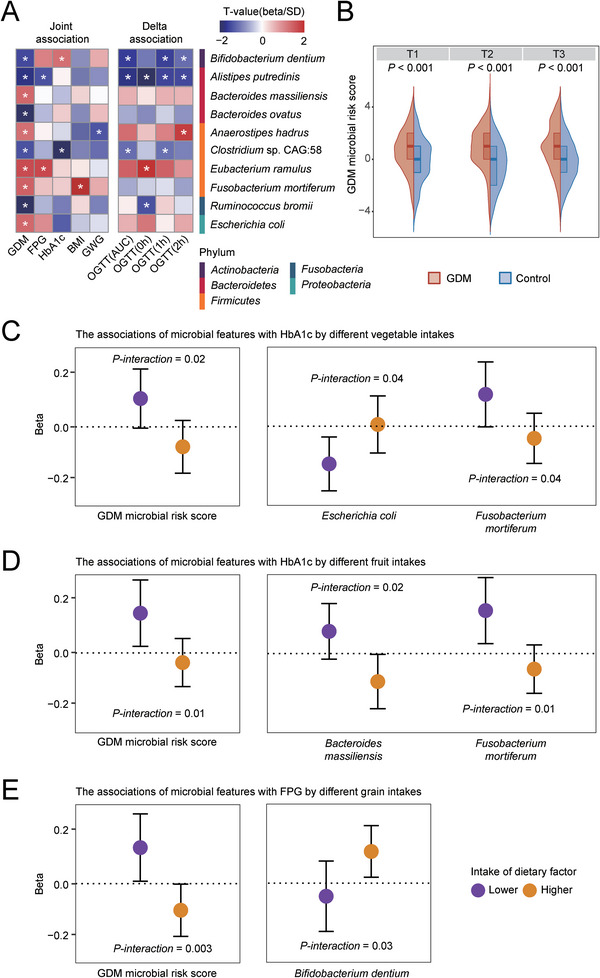
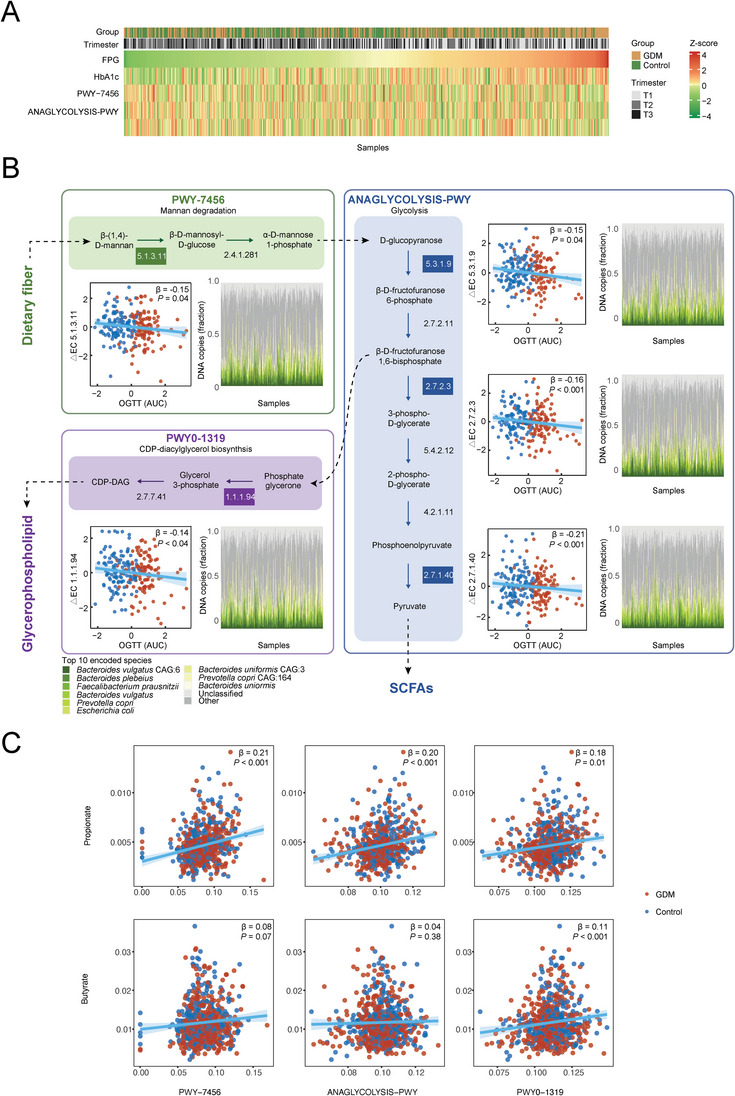
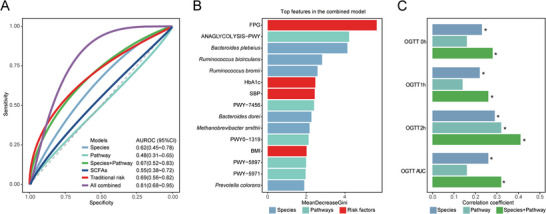
Though gut microbiome disturbance may be involved in the etiology of gestational diabetes mellitus (GDM), data on the gut microbiome's dynamic change during pregnancy and associations with gestational glucose metabolism are still inadequate. In this prospective study comprising 120 pairs of GDM patients and matched pregnant controls, a decrease in the diversity of gut microbial species and changes in the microbial community composition with advancing gestation are found in controls, while no such trends are observed in GDM patients. Multivariable analysis identifies 10 GDM-related species (e.g., Alistipes putredinis), and the integrated associations of these species with glycemic traits are modified by habitual intake of fiber-rich plant foods. In addition, the microbial metabolic potentials related to fiber fermentation (e.g., mannan degradation pathways) and their key enzymes consistently emerge as associated with both GDM status and glycemic traits. Microbial features especially those involved in fiber fermentation, provide an incremental predictive value in a prediction model with established risk factors of GDM. These data suggest that the gut microbiome remodeling with advancing gestation is different in GDM patients compared with controls, and dietary fiber fermentation contributes to the influence of gut microbiome on gestational glycemic regulation.
Keywords: gestational diabetes mellitus; glucose metabolism; gut microbiome; matched case-control study.
© 2023 The Authors. Advanced Science published by Wiley-VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources