

Kaposiform lymphangiomatosis: Diagnosis, pathogenesis, and treatment
- PMID: 36683202
- PMCID: PMC10018800
- DOI: 10.1002/pbc.30219
Kaposiform lymphangiomatosis: Diagnosis, pathogenesis, and treatment
Abstract
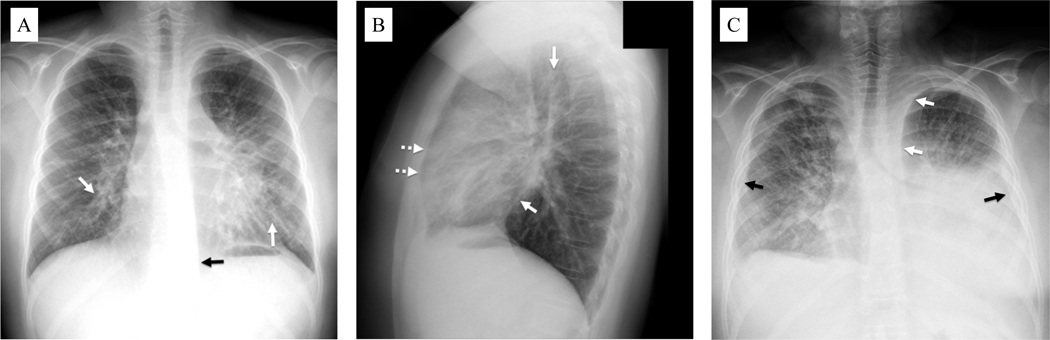
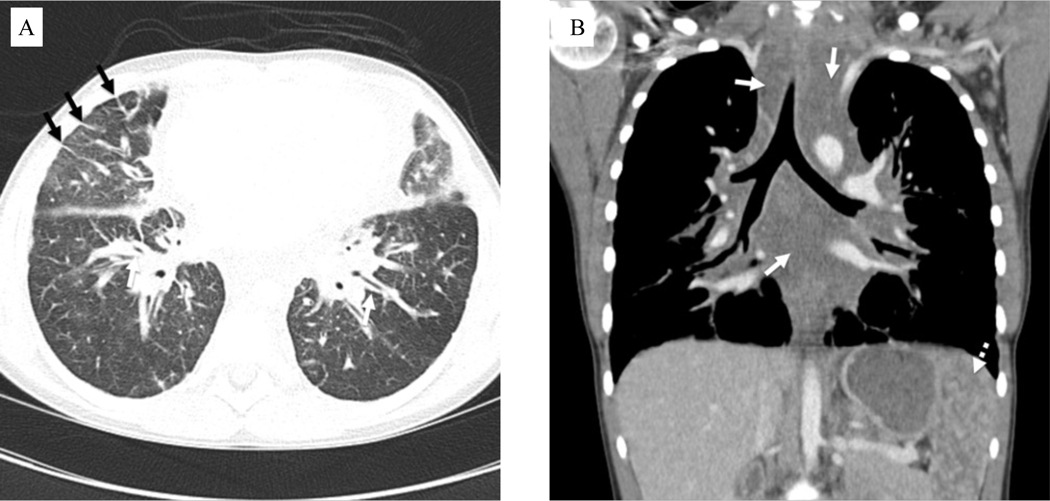
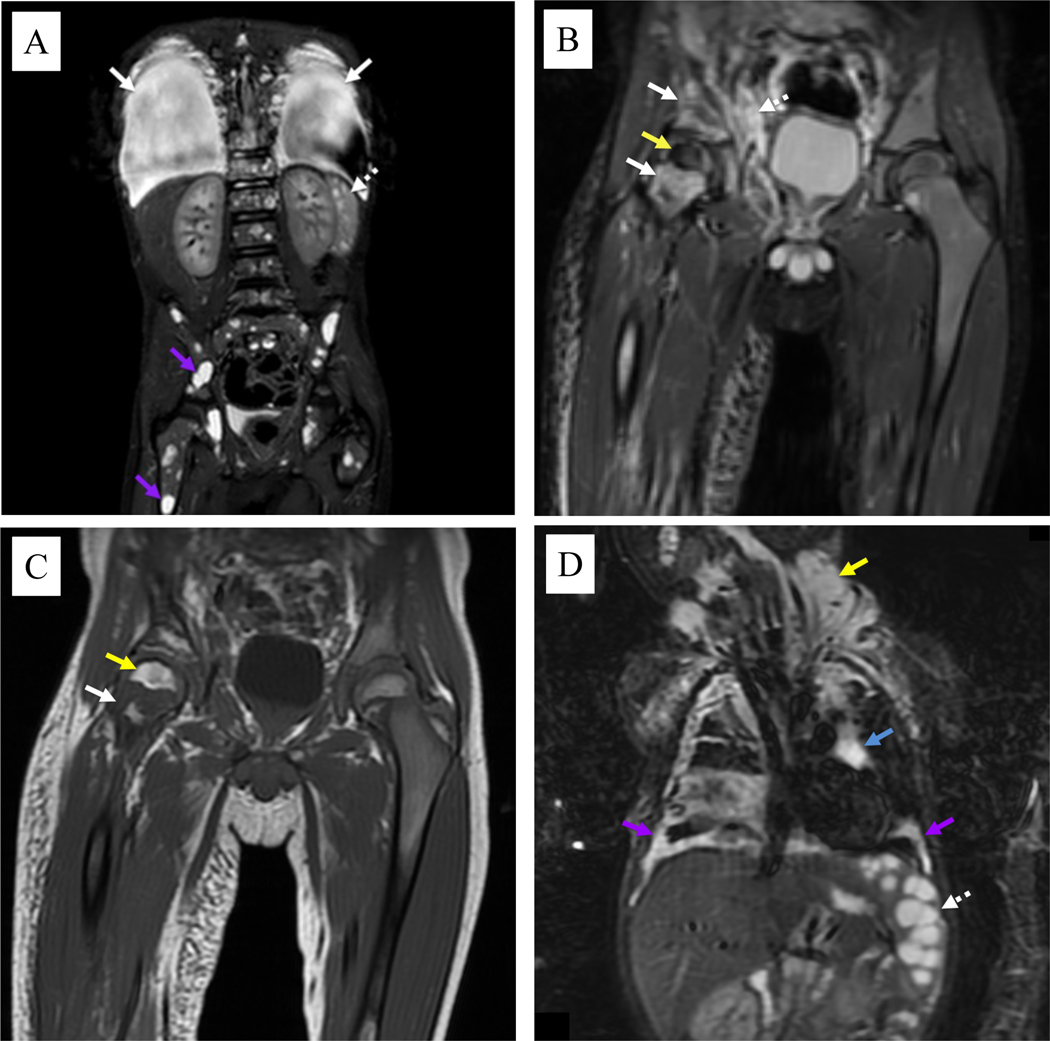
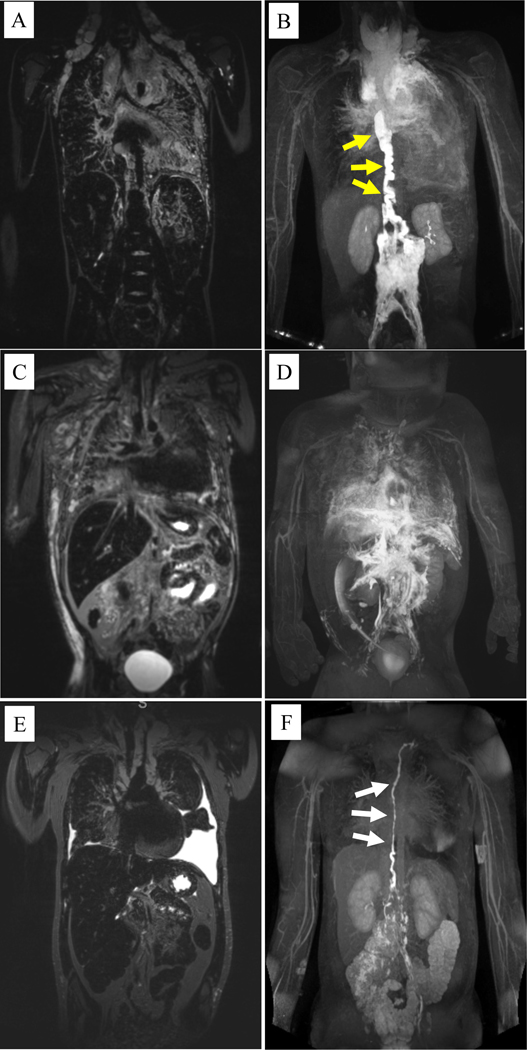
Kaposiform lymphangiomatosis (KLA) is a life-threatening rare disease that can cause substantial morbidity, mortality, and social burdens for patients and their families. Diagnosis often occurs long after initial symptoms, and there are few centers in the world with the expertise to diagnose and care for patients with the disease. KLA is a lymphatic anomaly and significant advancements have been made in understanding its pathogenesis and etiology since its first description in 2014. This review provides multidisciplinary, comprehensive, and state-of-the-art information on KLA patient presentation, diagnostic imaging, pathology, organ involvement, genetics, and pathogenesis. Finally, we describe current therapeutic approaches, important areas for research, and challenges faced by patients and their families. Further insights into the pathogenesis of KLA may advance our understanding of other vascular anomalies given that similar signaling pathways may be involved.
Keywords: kaposiform lymphangiomatosis; lymphatic anomalies; rare diseases.
© 2023 The Authors. Pediatric Blood & Cancer published by Wiley Periodicals LLC.
Conflict of interest statement
Figures
References
-
- Perez-Atayde AR, Debelenko L, Al-Ibraheemi A, et al. Kaposiform Lymphangiomatosis: Pathologic Aspects in 43 Patients. Am J Surg Pathol. 2022;46(7):963–976. - PubMed
-
- Fernandes VM, Fargo JH, Saini S, et al. Kaposiform lymphangiomatosis: unifying features of a heterogeneous disorder. Pediatr Blood Cancer. 2015;62(5):901–904. - PubMed
-
- Wang Z, Li K, Yao W, et al. Successful treatment of kaposiform lymphangiomatosis with sirolimus. Pediatric blood & cancer. 2015;62(7):1291–1293. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
