

Race, geography, and risk of breast cancer treatment delays: A population-based study 2004-2015
- PMID: 36683417
- PMCID: PMC11578059
- DOI: 10.1002/cncr.34573
Race, geography, and risk of breast cancer treatment delays: A population-based study 2004-2015
Abstract
Background: Treatment delays affect breast cancer survival and constitute poor-quality care. Black patients experience more treatment delay, but the relationship of geography to these disparities is poorly understood.
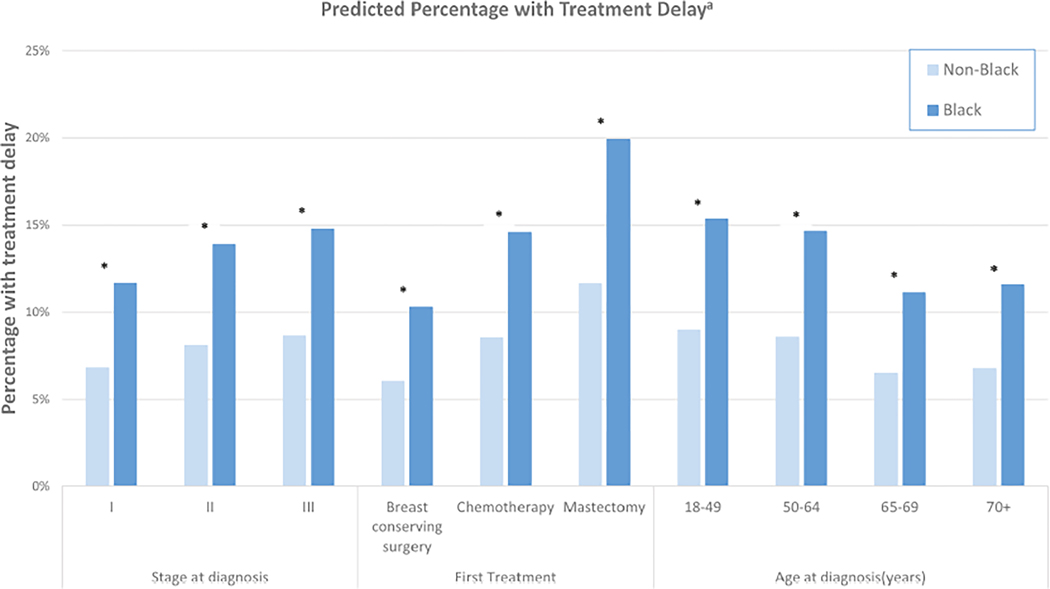
Methods: We studied a population-based, retrospective, observational cohort of patients with breast cancer in North Carolina between 2004 and 2017 from the Cancer Information and Population Health Resource, which links cancer registry and sociodemographic data to multipayer insurance claims. We included patients >18 years with Stage I-III breast cancer who received surgery or chemotherapy as their first treatment. Delay was defined as >60 days from diagnosis to first treatment. Counties were aggregated into nine Area Health Education Center regions. Race was dichotomized as Black versus non-Black.
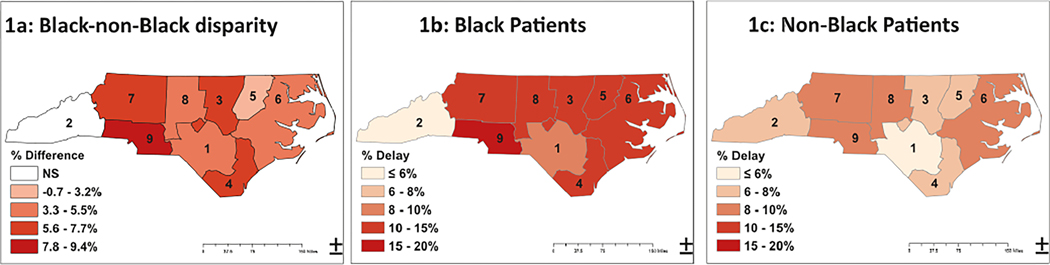
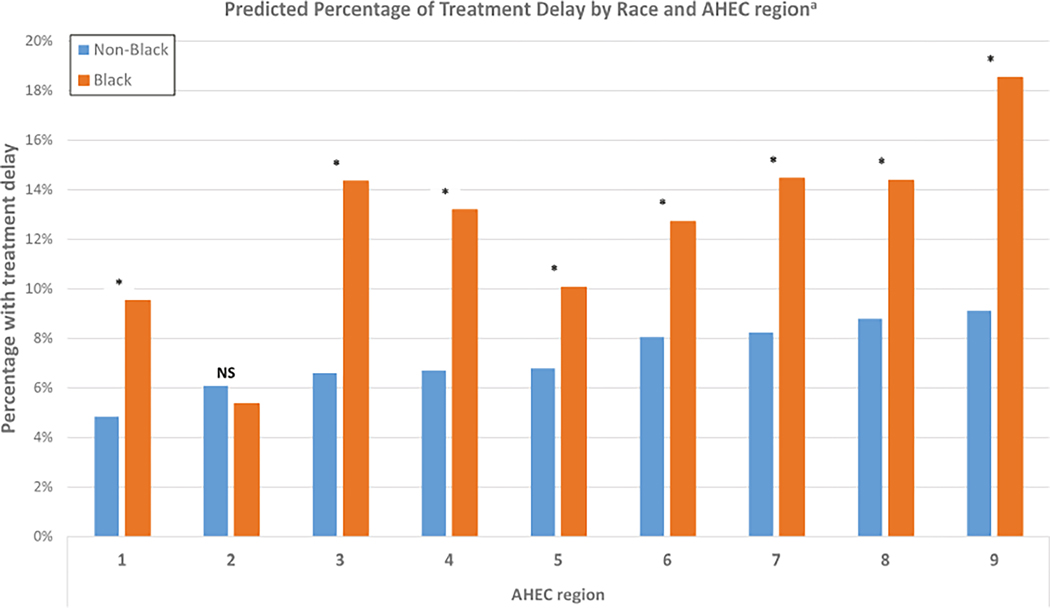
Results: Among 32,626 patients, 6190 (19.0%) were Black. Black patients were more likely to experience treatment delay >60 days (15.0% of Black vs. 8.0% of non-Black). Using race-stratified modified Poisson regression, age-adjusted relative risk of delay in the highest risk region was approximately twice that in the lowest risk region among Black (relative risk, 2.1; 95% CI, 1.6-2.6) and non-Black patients (relative risk, 1.9; 95% CI, 1.5-2.3). Adjustment for clinical and sociodemographic features only slightly attenuated interregion differences. The magnitude of the racial gap in treatment delay varied by region, from 0.0% to 9.4%.
Conclusions: Geographic region was significantly associated with risk of treatment delays for both Black and non-Black patients. The magnitude of racial disparities in treatment delay varied markedly between regions. Future studies should consider both high-risk geographic regions and high-risk patient groups for intervention to prevent delays.
Keywords: Breast Cancer; Cohort Study; Geographical Distribution; Racial Disparities; Treatment Initiation.
© 2023 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST
Katherine E. Reeder-Hayes and Stephanie B. Wheeler received unrelated grant funding paid to their institution by the Pfizer Medical Foundation. All other authors made no disclosures.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
