

A Network Meta-Analysis of Two Doses of Recombinant Human Thrombopoietin for Treating Sepsis-Related Thrombocytopenia
- PMID: 36683598
- PMCID: PMC9822753
- DOI: 10.1155/2022/2124019
A Network Meta-Analysis of Two Doses of Recombinant Human Thrombopoietin for Treating Sepsis-Related Thrombocytopenia
Abstract
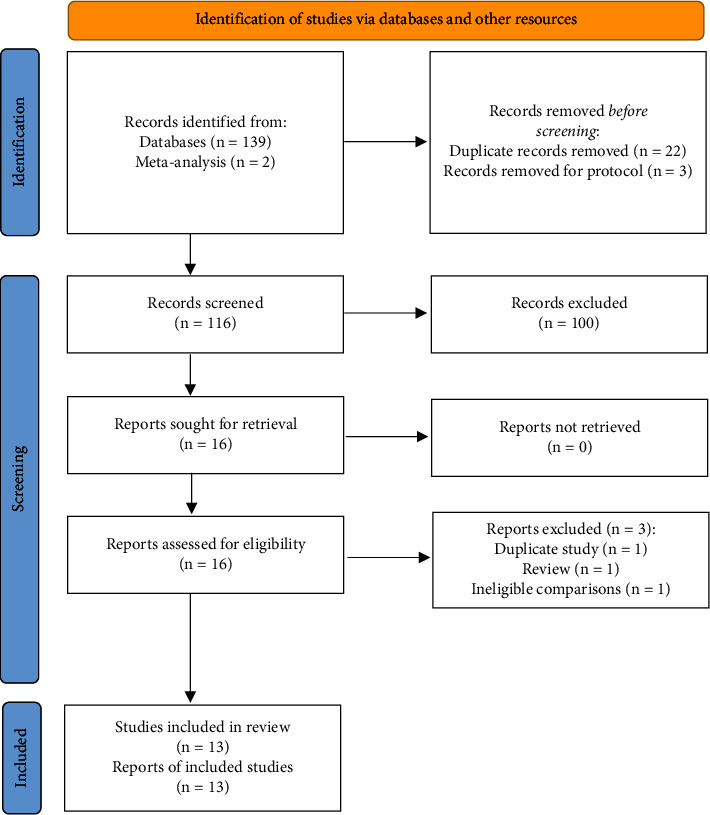
Previous studies suggest that sepsis remains a common critical illness with a global incidence of 31.5 million. The aim of this study was to evaluate the comparative therapeutic value of recombinant human thrombopoietin (rhTPO) in treating sepsis patients with thrombocytopenia. We conducted a comprehensive electronic search of PubMed, EMBASE, the Cochrane Library, and CNKI from its inception through December 31, 2021. Thirteen randomized controlled trials (RCTs) involving 963 patients were included. Network meta-analyses showed that rhTPO 300 U/kg/day and rhTPO 15000 U/day significantly increased the platelet (PLT) levels on the 7th day and decreased the requirement of transfusion of red blood cells (RBCs), plasma, and PLT compared with IVIG and NAT. SUCRA showed that rhTPO 300 U/kg/day ranked first in terms of 28-day mortality (85.5%) and transfusion, including RBC (88.7%), plasma (89.6%), and PLT (95.2%), while rhTPO 15000 U/day ranked first for the length of the intensive care unit (ICU) stay (95.9%) and PLT level at day 7 (91.6%). rhTPO 300 U/kg/day may be the optimal dose to reduce 28-day mortality and transfusion requirements. However, rhTPO 15000 U/day may be the optimal dose for shortening the ICU stay and increasing the PLT level on the 7th day. However, additional studies to further validate our findings are needed.
Copyright © 2022 Dandan Chen et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures





Similar articles
-
Efficacy and Safety of Recombinant Human Thrombopoietin (rhTPO) on Coagulation Function and Inflammatory Factors in the Treatment of Patients with Sepsis-Related Thrombocytopenia.Clin Appl Thromb Hemost. 2025 Jan-Dec;31:10760296251315173. doi: 10.1177/10760296251315173. Clin Appl Thromb Hemost. 2025. PMID: 39901742 Free PMC article. Clinical Trial.
-
[The role of recombinant human thrombopoietin in critically ill patients with sepsis-associated thrombocytopenia: a clinical study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Dec;32(12):1445-1449. doi: 10.3760/cma.j.cn121430-20201130-00737. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 33541495 Clinical Trial. Chinese.
-
The effect of recombinant human thrombopoietin (rhTPO) on sepsis patients with acute severe thrombocytopenia: a study protocol for a multicentre randomised controlled trial (RESCUE trial).BMC Infect Dis. 2019 Sep 6;19(1):780. doi: 10.1186/s12879-019-4388-2. BMC Infect Dis. 2019. PMID: 31492102 Free PMC article. Clinical Trial.
-
Efficacy and Safety of Recombinant Human Thrombopoietin on Sepsis Patients With Thrombocytopenia: A Systematic Review and Meta-Analysis.Front Pharmacol. 2020 Jun 24;11:940. doi: 10.3389/fphar.2020.00940. eCollection 2020. Front Pharmacol. 2020. PMID: 32714186 Free PMC article.
-
Clinical experience with recombinant human thrombopoietin in chemotherapy-induced thrombocytopenia.Semin Hematol. 2000 Apr;37(2 Suppl 4):28-34. doi: 10.1053/shem.2000.7391. Semin Hematol. 2000. PMID: 10831286 Review.
Cited by
-
Thrombocytopenia in the intensive care unit: diagnosis and management.Ann Intensive Care. 2025 Feb 22;15(1):25. doi: 10.1186/s13613-025-01447-x. Ann Intensive Care. 2025. PMID: 39985745 Free PMC article. Review.
References
-
- Schultz M. J., Dünser M. W., Dondorp A. M., et al. Current challenges in the management of sepsis in ICUs in resource-poor settings and suggestions for the future. In: Dondorp A. M., Dünser M. W., Schultz M. J., editors. Sepsis Management in Resource-Limited Settings . Heidelberger, Berlin: Springer Copyright; 2019. pp. 1–24. - PubMed
-
- Sharma B., Sharma M., Majumder M., Steier W., Sangal A., Kalawar M. Thrombocytopenia in septic shock patients--a prospective observational study of incidence, risk factors and correlation with clinical outcome. Anaesthesia & Intensive Care . 2007;35(6):874–880. doi: 10.1177/0310057x0703500604. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical