

Successful outcomes of unilateral vs bilateral pedicle screw fixation for lumbar interbody fusion: A meta-analysis with evidence grading
- PMID: 36683615
- PMCID: PMC9851015
- DOI: 10.12998/wjcc.v10.i36.13337
Successful outcomes of unilateral vs bilateral pedicle screw fixation for lumbar interbody fusion: A meta-analysis with evidence grading
Abstract
Background: Whether it's better to adopt unilateral pedicle screw (UPS) fixation or to use bilateral pedicle screw (BPS) one for lumbar degenerative diseases is still controversially undetermined.
Aim: To make a comparison between UPS and BPS fixation as to how they work efficaciously and safely in patients suffering from lumbar degenerative diseases.
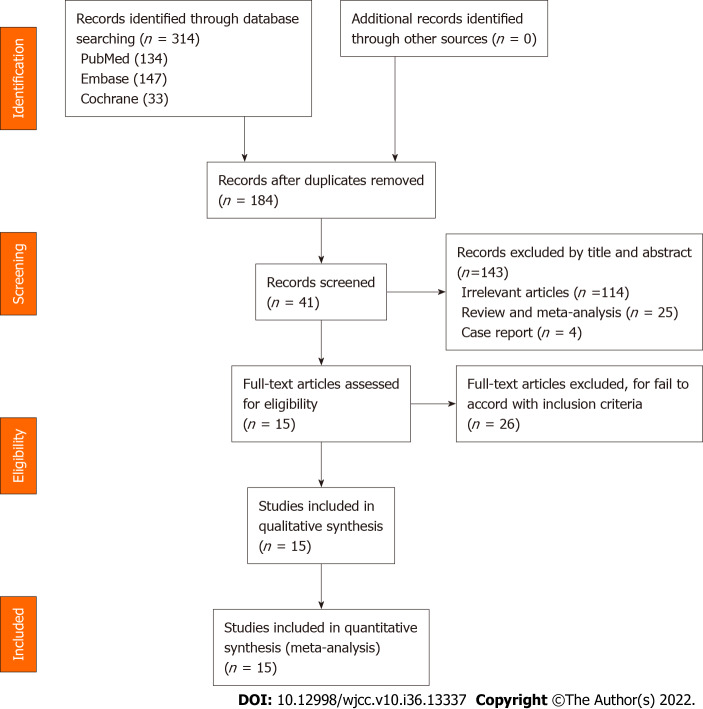
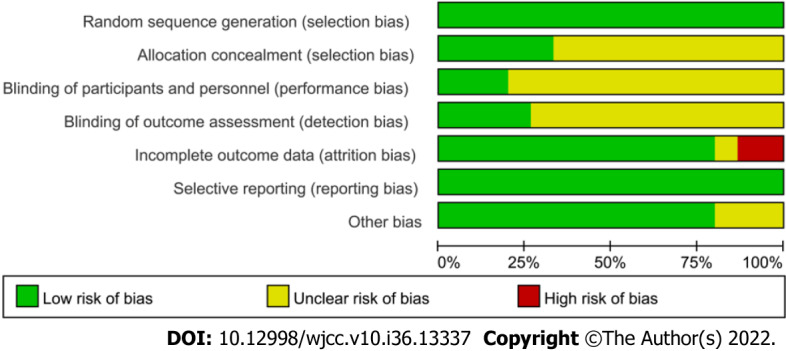
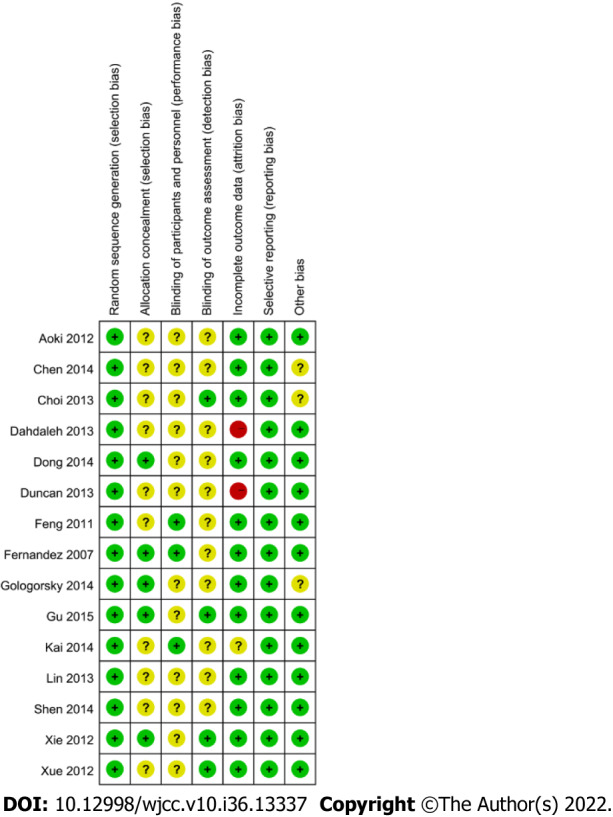
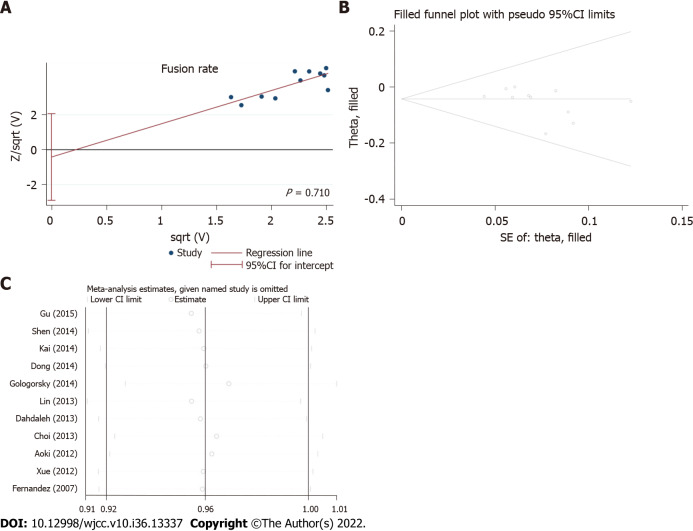
Methods: We have searched a lot in the databases through 2020 with index terms such as "unilateral pedicle screw fixation" and "bilateral pedicle screw fixation." Only randomized controlled trials and some prospective cohort studies could be found, yielding 15 studies. The intervention was unilateral pedicle screw fixation; Primarily We've got outcomes of complications and fusion rates. Secondarily, we've achieved outcomes regarding total blood loss, operative time, as well as length of stay. Softwares were installed and utilized for subgroup analysis, analyzing forest plots, sensitivity, heterogeneity, forest plots, publication bias, and risk of bias.
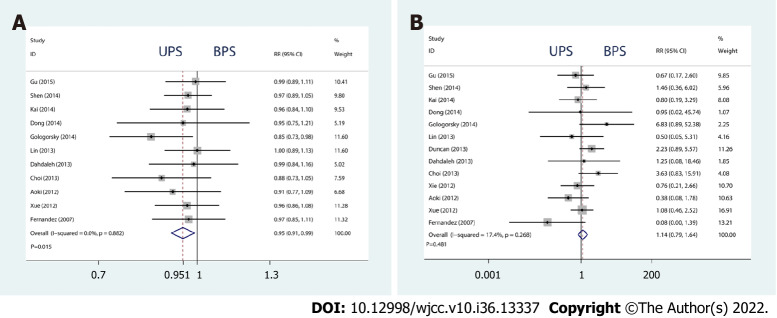
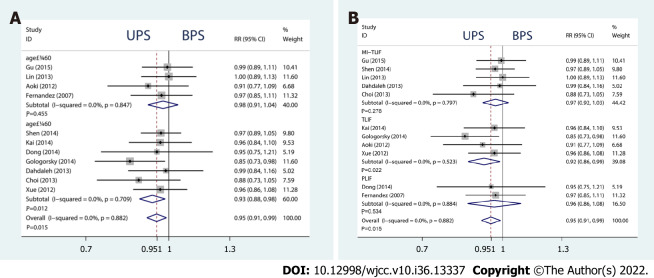
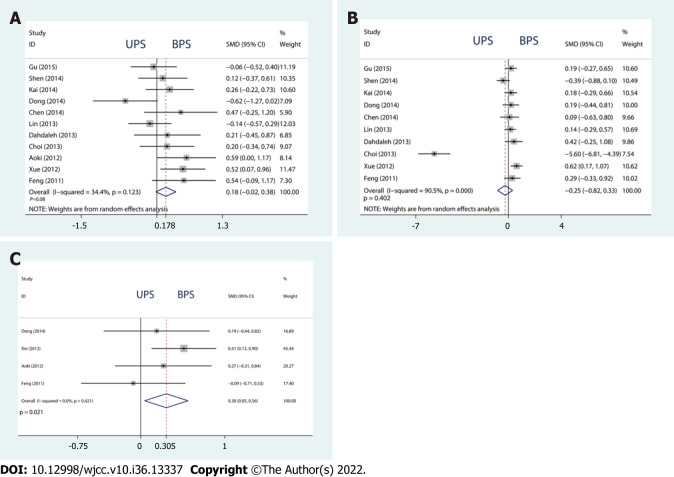
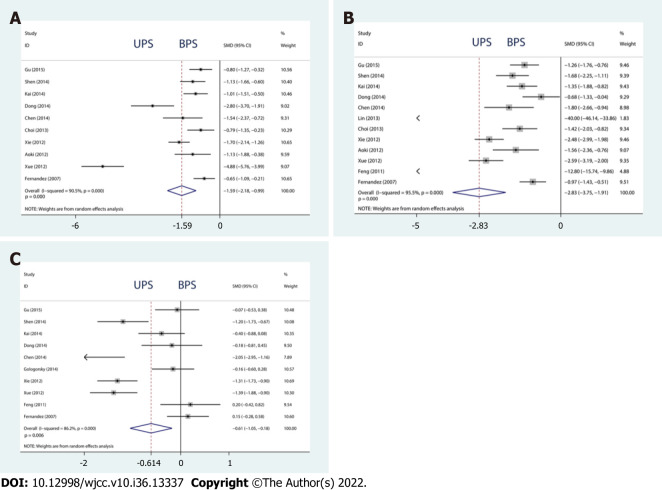
Results: Fifteen previous cases of study including 992 participants have been involved in our meta-analysis. UPS had slightly lower effects on fusion rate [relative risk (RR) = 0.949, 95%CI: 0.910 to 0.990, P = 0.015], which contributed mostly to this meta-analysis, and similar complication rates (RR = 1.140, 95%CI: 0.792 to 1.640, P = 0.481), Δ visual analog scale [standard mean difference (SMD) = 0.178, 95%CI: -0.021 to 0.378, P = 0.080], and Δ Oswestry disability index (SMD = -0.254, 95%CI: -0.820 to 0.329, P = 0.402). In contrast, an obvious difference has been observed in Δ Japanese Orthopedic Association (JOA) score (SMD = 0.305, 95%CI: 0.046 to 0.563, P = 0.021), total blood loss (SMD = -1.586, 95%CI: -2.182 to -0.990, P = 0.000), operation time (SMD = -2.831, 95%CI: -3.753 to -1.909, P = 0.000), and length of hospital stay (SMD = -0.614, 95%CI: -1.050 to -0.179, P = 0.006).
Conclusion: Bilateral fixation is more effective than unilateral fixation regarding fusion rate after lumbar interbody fusion. However, JOA, operation time, total blood loss, as well as length of stay were improved for unilateral fixation.
Keywords: Bilateral pedicle screw fixation; Discectomy; Lumbar interbody fusion; Meta-analysis; Spinal fusion surgery; Unilateral pedicle screw fixation.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no competing interests.
Figures
References
-
- Hibbs RA. An operation for progressive spinal deformities: a preliminary report of three cases from the service of the orthopaedic hospital. 1911. Clin Orthop Relat Res. 2007;460:17–20. - PubMed
-
- Cho JY, Goh TS, Son SM, Kim DS, Lee JS. Comparison of Anterior Approach and Posterior Approach to Instrumented Interbody Fusion for Spondylolisthesis: A Meta-analysis. World Neurosurg. 2019;129:e286–e293. - PubMed
-
- Levin JM, Tanenbaum JE, Steinmetz MP, Mroz TE, Overley SC. Posterolateral fusion (PLF) versus transforaminal lumbar interbody fusion (TLIF) for spondylolisthesis: a systematic review and meta-analysis. Spine J. 2018;18:1088–1098. - PubMed
LinkOut - more resources
Full Text Sources
