

Staphylococcus aureus bacteremia and infective endocarditis in a patient with epidermolytic hyperkeratosis: A case report
- PMID: 36683620
- PMCID: PMC9850991
- DOI: 10.12998/wjcc.v10.i36.13418
Staphylococcus aureus bacteremia and infective endocarditis in a patient with epidermolytic hyperkeratosis: A case report
Abstract
Background: Staphylococcus aureus bacteraemia (SAB) is among the leading causes of bacteraemia and infectious endocarditis. The frequency of infectious endocarditis (IE) among SAB patients ranges from 5% to 10%-12%. In adults, the characteristics of epidermolytic hyperkeratosis (EHK) include hyperkeratosis, erosions, and blisters. Patients with inflammatory skin diseases and some diseases involving the epidermis tend to exhibit a disturbed skin barrier and tend to have poor cell-mediated immunity.
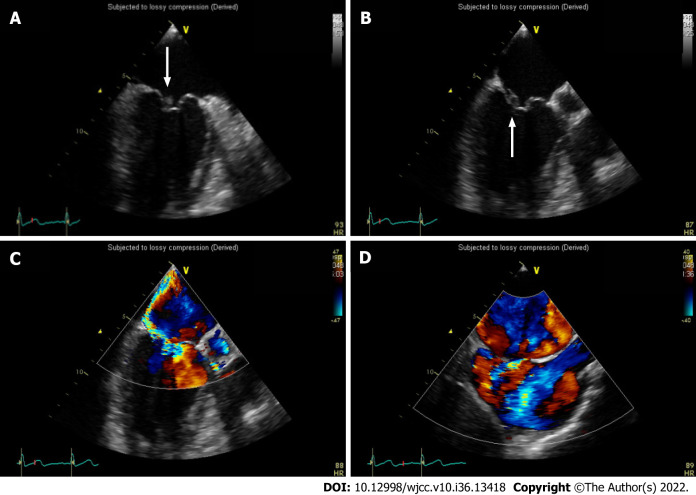
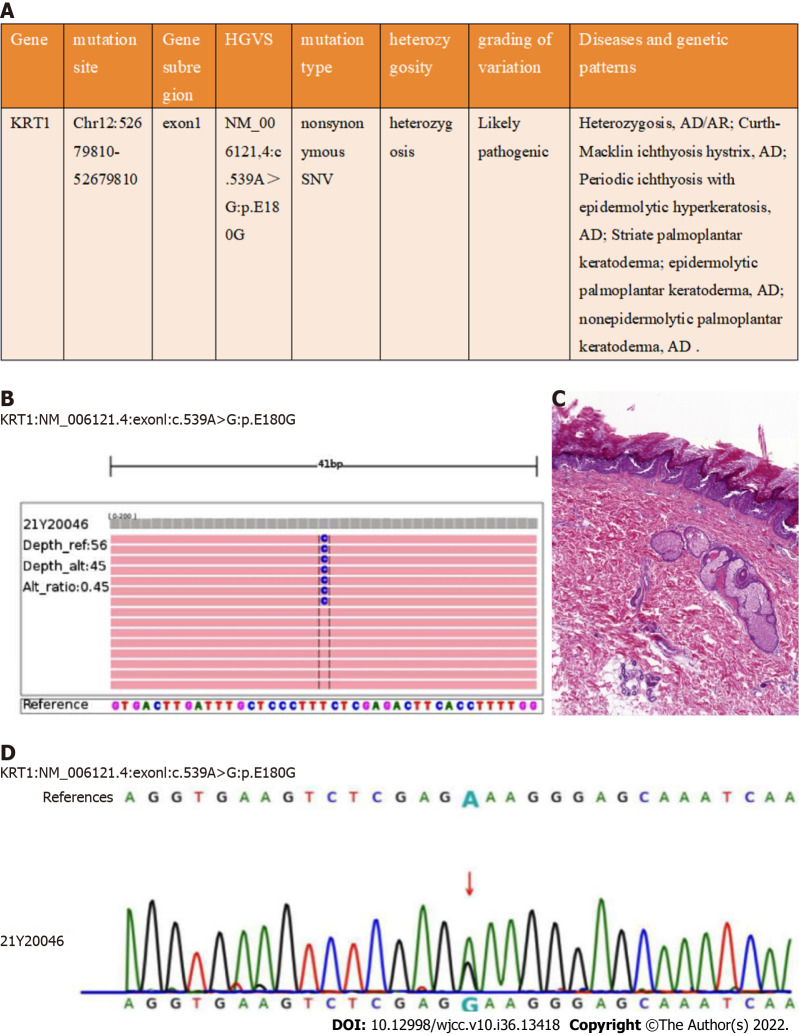
Case summary: We describe a case of SAB and infective endocarditis in a 43-year-old male who presented with fever of unknown origin and skin diseases. After genetic tests, the skin disease was diagnosed as EHK.
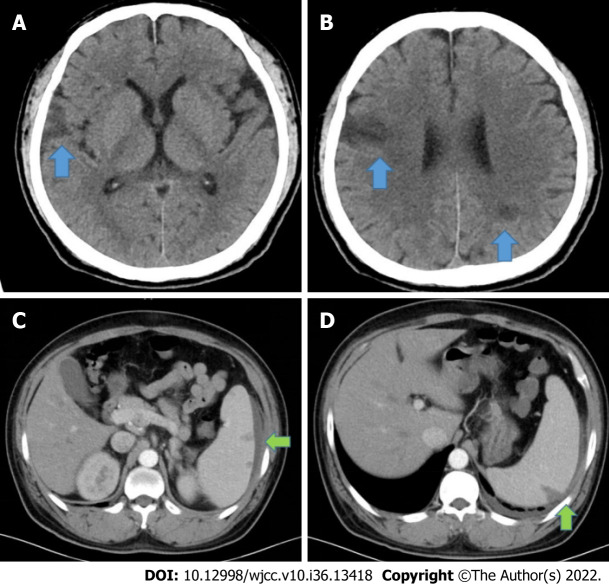
Conclusion: A breached skin barrier secondary to EHK, coupled with inadequate sanitation, likely provided the opportunity for bacterial seeding, leading to IE and deep-seated abscess or organ abscess. EHK may be associated with skin infection and multiple risk factors for extracutaneous infections. Patients with EHK should be treated early to minimize their consequences. If patients with EHK present with prolonged fever of unknown origin, IE and organ abscesses should be ruled out, including metastatic spreads.
Keywords: Case report; Epidermolytic hyperkeratosis; Infective endocarditis; Staphylococcus aureus bacteremia.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work, there is no professional or other personal interest of any nature or kind in any product, service and/or company that could be construed as influencing the position presented in, or the review of, the manuscript entitled.
Figures

Similar articles
-
A recurrent missense mutation of keratin 1 gene in a Chinese family with epidermolytic hyperkeratosis (severe palmoplantar hyperkeratosis, type 1).Int J Dermatol. 2012 Feb;51(2):182-5. doi: 10.1111/j.1365-4632.2011.05202.x. Int J Dermatol. 2012. PMID: 22250628
-
Staphylococcus aureus bacteremia in the surgical patient: a prospective analysis of 73 postoperative patients who developed Staphylococcus aureus bacteremia at a tertiary care facility.J Am Coll Surg. 2000 Jan;190(1):50-7. doi: 10.1016/s1072-7515(99)00211-2. J Am Coll Surg. 2000. PMID: 10625232
-
Epidermolytic hyperkeratosis type NPS-3: a case report.Acta Dermatovenerol Croat. 2007;15(1):20-3. Acta Dermatovenerol Croat. 2007. PMID: 17433175
-
Vulvar Epidermolytic Hyperkeratosis: A Comprehensive Systematic Review of Case Reports and Series.J Clin Med. 2024 Dec 27;14(1):94. doi: 10.3390/jcm14010094. J Clin Med. 2024. PMID: 39797176 Free PMC article. Review.
-
Epidermolytic Hyperkeratosis in an Epidermoid (Infundibular) Cyst.Am J Dermatopathol. 2022 Mar 1;44(3):215-217. doi: 10.1097/DAD.0000000000002098. Am J Dermatopathol. 2022. PMID: 34966043 Review.
References
-
- Miao H, Dong R, Zhang S, Yang L, Liu Y, Wang T. Inherited ichthyosis and fungal infection: an update on pathogenesis and treatment strategies. J Dtsch Dermatol Ges. 2021;19:341–350. - PubMed
-
- Rice AS, Crane JS. Epidermolytic Hyperkeratosis. [Updated 2022 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544323/ - PubMed
-
- Kurosawa M, Takagi A, Tamakoshi A, Kawamura T, Inaba Y, Yokoyama K, Kitajima Y, Aoyama Y, Iwatsuki K, Ikeda S. Epidemiology and clinical characteristics of bullous congenital ichthyosiform erythroderma (keratinolytic ichthyosis) in Japan: results from a nationwide survey. J Am Acad Dermatol. 2013;68:278–283. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
