

Accuracy of post-operative recall by degenerative cervical myelopathy patients using the modified Japanese Orthopaedic Association scale
- PMID: 36683652
- PMCID: PMC9844220
Accuracy of post-operative recall by degenerative cervical myelopathy patients using the modified Japanese Orthopaedic Association scale
Abstract
Background and aim: The modified Japanese Orthopaedic Association (mJOA) scale is one of the primary measures of neurological function used on patients with degenerative cervical myelopathy (DCM). Contrary to some reports, the mJOA is not based on patient-reported outcomes as it is an assessment conducted by physicians, allied health professionals, or trained staff. To date, the accuracy of post-operative recall by DCM patients of their pre-operative neurological function, as assessed by the mJOA scale, has not been examined. This study, therefore, aimed to evaluate recall accuracy in DCM patients using the mJOA scale.
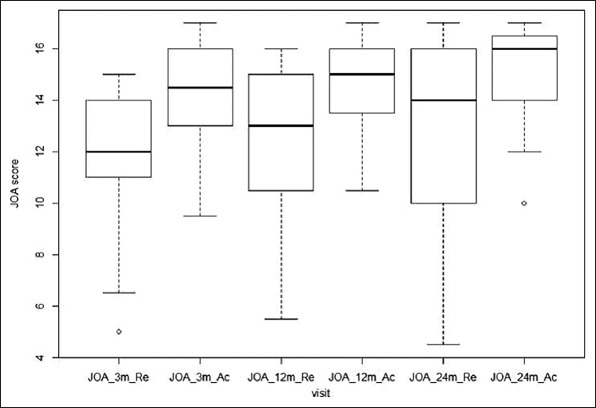
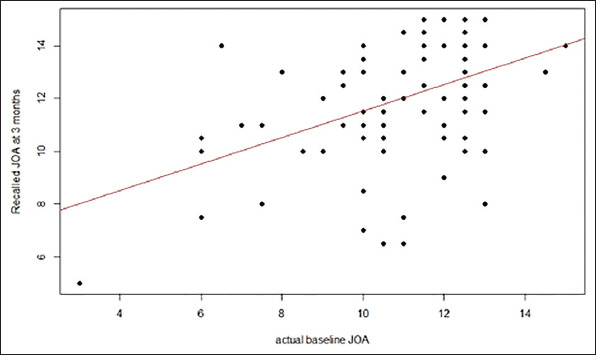
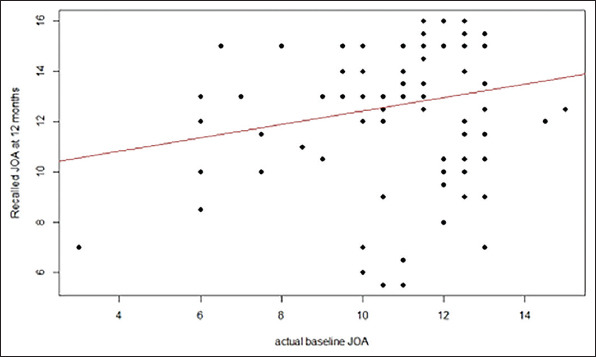
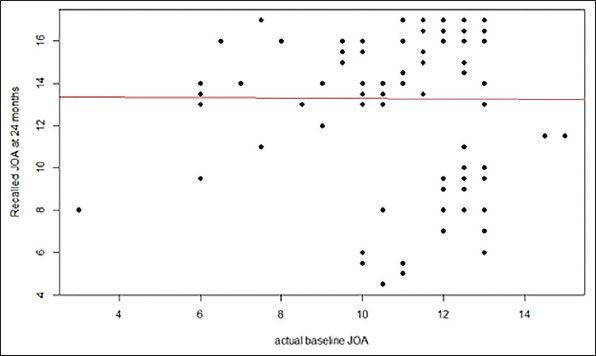
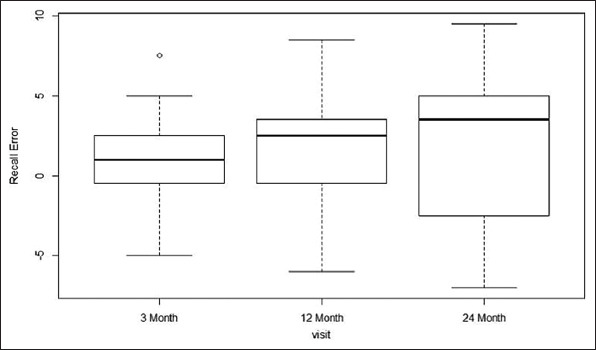
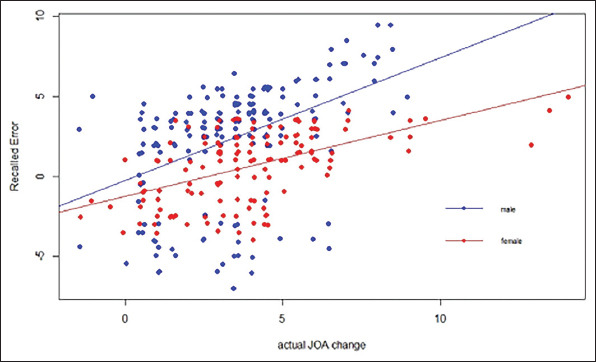
Methods: This study analyzed recall capacity of DCM patients who had undergone anterior cervical discectomy and fusion by a single surgeon at a large academic spine center between February 2012 and August 2017. Patient recall of neurological function pre-surgery was assessed at 3, 12, and 24 months post-surgery using the mJOA scale. Actual mJOA scores were also determined at each follow-up. Recall error (RE) was defined as the difference between recalled mJOA score at each post-operative visit and the actual baseline score. Age, gender, surgical segments, hospital length of stay, actual mJOA scores at follow-up, and actual rate of improvement in mJOA score were analyzed as predictors of recall accuracy. Descriptive statistics were collected to profile the characteristics of patients enrolled in the study cohort. All statistical computing and graphing were performed with R software and generalized estimating equation (GEE) model fitting was done using geepack package.
Results: A total of 105 patients (56.2% of males and 43.8% of females) were enrolled in the study. The median ± SD (range) age at the pre-surgical baseline measurement was 50 ± 8 (25 - 78) years. The recalled mJOA scores at the three follow-up time points were lower than the actual mJOA scores. The recall accuracy gradually decreased over time. Estimated coefficients showed that all variables in the GEE model except for surgical fusion segments were significant (P < 0.05). The pre-operative actual baseline mJOA score was inversely associated with RE. An increasing actual mJOA score over time had a significant positive influence on RE. Greater RE was found in males compared to females. Unexpectedly, age was inversely associated with RE.
Conclusions: The RE increases with the time interval between pre-surgical measurement and post-surgical follow-up and is more prominent in male DCMs patients following upper spine surgery.
Relevance for patients: It is necessary to select post-operative patients who need to pay attention according to the three factors of post-operative time, gender, and age, that is, patients with large RE should be given early or timely psychological counseling and treatment concerns, so as to reduce the occurrence of potential medical disputes and improve the level of medical safety.
Keywords: anterior cervical discectomy; degenerative cervical myelopathy; intervertebral fusion; neurological function; patient-reported outcomes; recall error.
Copyright: © 2022 Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
A Retrospective Study of Degenerative Cervical Myelopathy and the Surgical Management Within Northern Ireland.Cureus. 2023 Nov 27;15(11):e49513. doi: 10.7759/cureus.49513. eCollection 2023 Nov. Cureus. 2023. PMID: 38024056 Free PMC article.
-
The Pre-Operative Duration of Symptoms: The Most Important Predictor of Post-Operative Efficacy in Patients with Degenerative Cervical Myelopathy.Brain Sci. 2022 Aug 17;12(8):1088. doi: 10.3390/brainsci12081088. Brain Sci. 2022. PMID: 36009151 Free PMC article.
-
Predicting the minimum clinically important difference in patients undergoing surgery for the treatment of degenerative cervical myelopathy.Neurosurg Focus. 2016 Jun;40(6):E14. doi: 10.3171/2016.3.FOCUS1665. Neurosurg Focus. 2016. PMID: 27246484
-
Predictors of Outcome After Surgical Decompression for mild degenerative Cervical Myelopathy -A Systematic Review.Global Spine J. 2024 Mar;14(2):697-706. doi: 10.1177/21925682231164346. Epub 2023 Mar 13. Global Spine J. 2024. PMID: 36912895 Free PMC article. Review.
-
Gait assessment tools for degenerative cervical myelopathy: a systematic review.J Spine Surg. 2022 Mar;8(1):149-162. doi: 10.21037/jss-21-109. J Spine Surg. 2022. PMID: 35441108 Free PMC article. Review.
References
-
- McCormick JD, Werner BC, Shimer AL. Patient-Reported Outcome Measures in Spine Surgery. J Am Acad Orthop Surg. 2013;21:99–107. - PubMed
-
- Coughlin SS. Recall Bias in Epidemiologic Studies. J Clin Epidemiol. 1990;43:87–91. - PubMed
-
- Howell J, Xu M, Duncan CP, Masri BA, Garbuz DS. A Comparison between Patient Recall and Concurrent Measurement of Preoperative Quality of Life Outcome in Toal Hip Arthroplasty. J Arthroplasty. 2008;23:843–9. - PubMed
-
- Lingard EA, Wright EA, Sledge CB, Kinemax Outcomes Group. Pitfalls of using Patient Recall to Derive Preoperative Status in Outcome Studies of Total Knee Arthroplasty. J Bone Joint Surg Am. 2001;83:1149–56. - PubMed
LinkOut - more resources
Full Text Sources