

Premedication before laryngoscopy in neonates: Evidence-based statement from the French society of neonatology (SFN)
- PMID: 36683794
- PMCID: PMC9846576
- DOI: 10.3389/fped.2022.1075184
Premedication before laryngoscopy in neonates: Evidence-based statement from the French society of neonatology (SFN)
Abstract
Context: Laryngoscopy is frequently required in neonatal intensive care. Awake laryngoscopy has deleterious effects but practice remains heterogeneous regarding premedication use. The goal of this statement was to provide evidence-based good practice guidance for clinicians regarding premedication before tracheal intubation, less invasive surfactant administration (LISA) and laryngeal mask insertion in neonates.
Methods: A group of experts brought together by the French Society of Neonatology (SFN) addressed 4 fields related to premedication before upper airway access in neonates: (1) tracheal intubation; (2) less invasive surfactant administration; (3) laryngeal mask insertion; (4) use of atropine for the 3 previous procedures. Evidence was gathered and assessed on predefined questions related to these fields. Consensual statements were issued using the GRADE methodology.
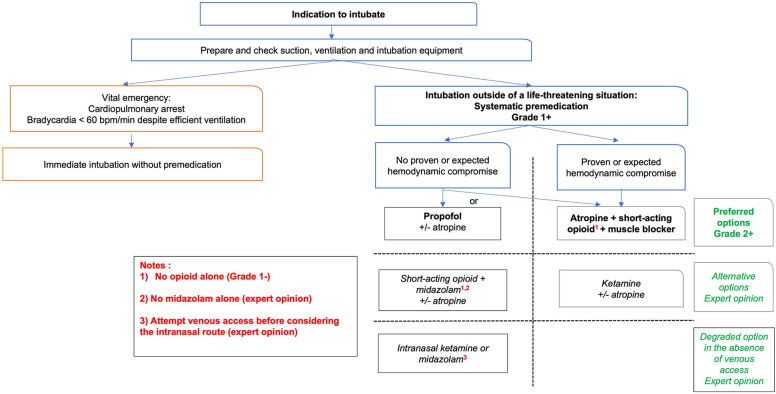
Results: Among the 15 formalized good practice statements, 2 were strong recommendations to do (Grade 1+) or not to do (Grade 1-), and 4 were discretionary recommendations to do (Grade 2+). For 9 good practice statements, the GRADE method could not be applied, resulting in an expert opinion. For tracheal intubation premedication was considered mandatory except for life-threatening situations (Grade 1+). Recommended premedications were a combination of opioid + muscle blocker (Grade 2+) or propofol in the absence of hemodynamic compromise or hypotension (Grade 2+) while the use of a sole opioid was discouraged (Grade 1-). Statements regarding other molecules before tracheal intubation were expert opinions. For LISA premedication was recommended (Grade 2+) with the use of propofol (Grade 2+). Statements regarding other molecules before LISA were expert opinions. For laryngeal mask insertion and atropine use, no specific data was found and expert opinions were provided.
Conclusion: This statement should help clinical decision regarding premedication before neonatal upper airway access and favor standardization of practices.
Keywords: analgeisa; anesthesia; atropine; intubation (intratracheal); laryngeal mask; less invasive surfactant administration (LISA); neonate; sedation.
© 2023 Durrmeyer, Walter-Nicolet, Chollat, Chabernaud, Barois, Chary Tardy, Berenguer, Bedu, Zayat, Roué, Beissel, Bellanger, Desenfants, Boukhris, Loose, Massudon Tagny, Chevallier, Milesi and Tauzin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous