

Laparoscopic restorative proctocolectomy with ileal-J-pouch anal canal anastomosis without diverting ileostomy for total colonic and extensive aganglionosis is safe and feasible with combined Lugol's iodine staining technique and indocyanine green fluorescence angiography
- PMID: 36683800
- PMCID: PMC9853408
- DOI: 10.3389/fped.2022.1090336
Laparoscopic restorative proctocolectomy with ileal-J-pouch anal canal anastomosis without diverting ileostomy for total colonic and extensive aganglionosis is safe and feasible with combined Lugol's iodine staining technique and indocyanine green fluorescence angiography
Abstract
Background: We present the surgical technique and outcomes of reduced-port laparoscopic restorative proctocolectomy with ileal-J-pouch anal canal anastomosis (IPACA) without diverting ileostomy for total colonic and extensive aganglionosis (TCA+).
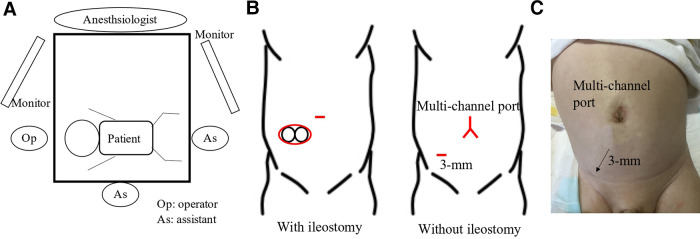
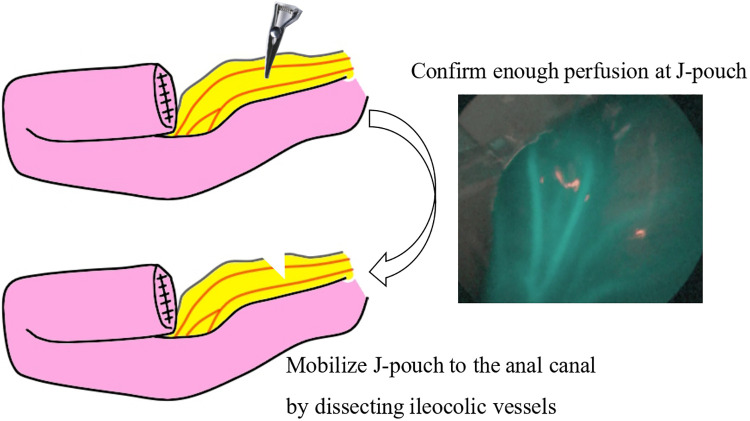
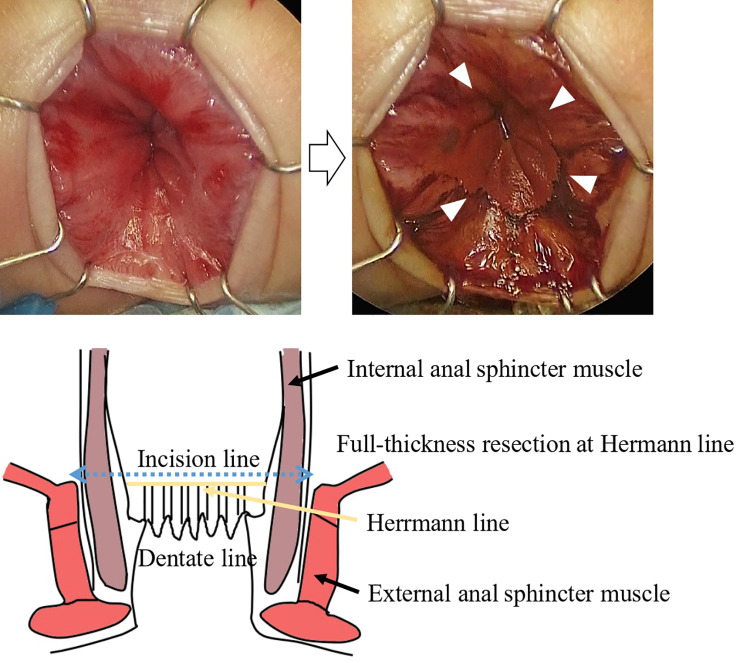
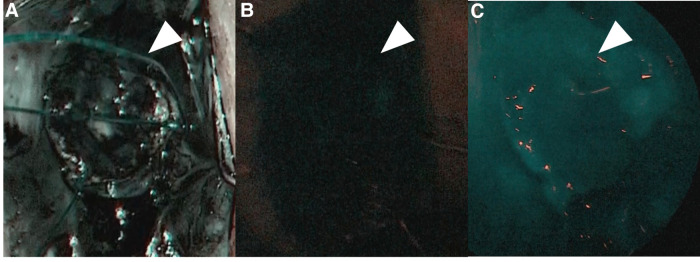
Methods: We retrospectively reviewed TCA+ cases between 2014 and 2022. Preoperative ileostomy was performed when transanal bowel irrigation was ineffective. Radical surgery for TCA+ was performed at approximately 6 kg. The surgery was performed using laparoscopy through a multi-channel trocar with or without an additional 3-mm trocar and IPACA reconstruction with indocyanine green fluorescence angiography (ICG) to assess anastomotic perfusion and Lugol's iodine staining to visualize the surgical anal canal.
Results: Ten patients with TCA+ were included. Ileostomy was performed in seven cases. The median operation time and blood loss were 274.5 min and 20 ml, respectively. No significant postoperative complications were found. All patients experienced frequent liquid stools and perianal excoriation in the early postoperative period, requiring anti-flatulence or codeine. The median follow-up period was 3.5 years. Three patients required irrigation management 1 year postoperatively, and the others defecated a median of 3.5 times per day. The median Kelly's clinical score was 5 in 5 patients aged >4 years.
Conclusion: Reduced-port surgery, combined with Lugol's iodine staining and ICG, was safe, feasible, and had cosmetically and clinically acceptable mid-term outcomes.
Keywords: diverting ileostomy; extensive aganglionosis; j pouch; laparoscopic restorative proctocolectomy; minimally invasive surgery; total colonic aganglionosis.
© 2023 Nakagawa, Yokota, Uchida, Hinoki, Shirota, Tainaka, Sumida, Makita, Amano, Takimoto, Ogata, Takada, Maeda and Gohda.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Reduced-port laparoscopic restorative proctocolectomy without diverting ileostomy.Asian J Endosc Surg. 2015 Nov;8(4):487-90. doi: 10.1111/ases.12201. Asian J Endosc Surg. 2015. PMID: 26708593
-
A novel Lugol's iodine staining technique to visualize the upper margin of the surgical anal canal intraoperatively for Hirschsprung disease: a case series.BMC Surg. 2020 Dec 4;20(1):317. doi: 10.1186/s12893-020-00986-3. BMC Surg. 2020. PMID: 33276766 Free PMC article.
-
Multimedia article. Laparoscopic ultralow anterior resection with colonic J-pouch-anal anastomosis.Dis Colon Rectum. 2008 Nov;51(11):1710-1. doi: 10.1007/s10350-008-9322-4. Epub 2008 Aug 5. Dis Colon Rectum. 2008. PMID: 18679748
-
Laparoscopic restorative proctocolectomy technical notes and postoperative results.Acta Chir Iugosl. 2012;59(2):39-45. doi: 10.2298/aci1202039b. Acta Chir Iugosl. 2012. PMID: 23373357 Review.
-
Ileal pouch-anal anastomosis: Points of controversy.J Visc Surg. 2014 Sep;151(4):281-8. doi: 10.1016/j.jviscsurg.2014.05.004. Epub 2014 Jul 3. J Visc Surg. 2014. PMID: 24999229 Review.
Cited by
-
Preoperative management comprising tube irrigation using a trans-anal indwelling tube for infants with hirschsprung disease can allow single-stage radical surgery.BMC Surg. 2023 Nov 1;23(1):333. doi: 10.1186/s12893-023-02232-y. BMC Surg. 2023. PMID: 37915052 Free PMC article.
-
Utilization of Indocyanine Green (ICG) Fluorescence in Patients with Pediatric Colorectal Diseases: The Current Applications and Reported Outcomes.Children (Basel). 2024 May 29;11(6):665. doi: 10.3390/children11060665. Children (Basel). 2024. PMID: 38929244 Free PMC article. Review.
References
-
- Dindo D, Demartines N, Clavien P-A. Classification of surgical complications. Ann Surg. (2004) 240:205–13. 10.1097/01.sla.0000133083.54934.ae. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources