

Reverse Peroneal Artery Flap-A Workhorse Flap for Reconstruction of Large, Distal Defects of Ankle and Foot
- PMID: 36683885
- PMCID: PMC9859685
- DOI: 10.1055/s-0042-1760091
Reverse Peroneal Artery Flap-A Workhorse Flap for Reconstruction of Large, Distal Defects of Ankle and Foot
Abstract
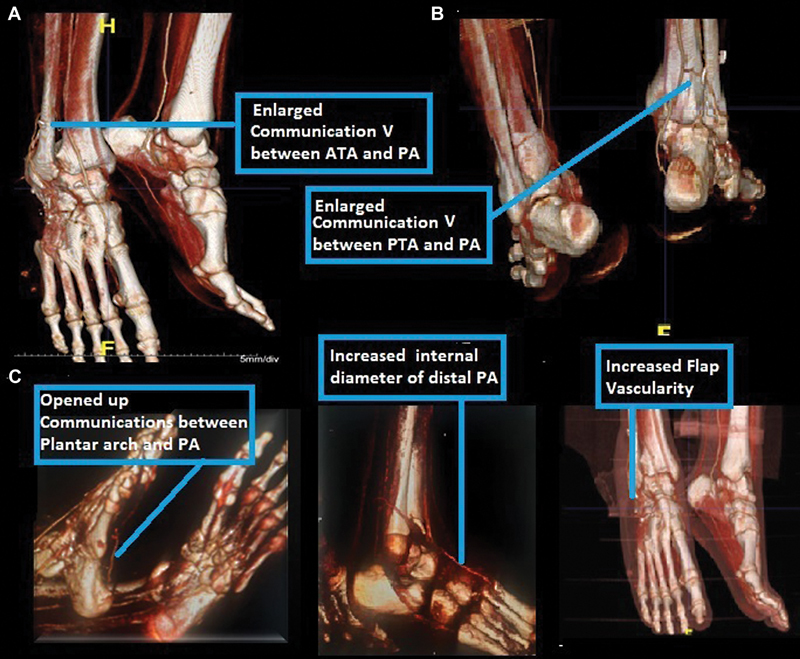
Background Reconstruction of large foot and ankle defects is a difficult task due to less available local soft tissue and more critical from functional point of view. To overcome the limitations associated with locoregional flaps and free flaps, reverse peroneal artery (RPA) flap was selected and its usefulness in reconstruction of distal large defects of the ankle and foot and its complications were studied. Materials and Methods This is a prospective observational study done in 20 patients treated as cohort within 2 years and 8 months from January 2018 to August 2020. Large defects of foot and ankle were reconstructed with RPA flap and evaluated for its usefulness. Three cases were evaluated with computed tomography angiography postoperatively, to assess the vascular pattern. Conclusion RPA flap is a versatile and very reliable flap for the reconstruction of large and distal defects of foot and ankle. It is safely done in children and in acute trauma without any major complications.
Keywords: CT peripheral angiogram; peroneal artery communications; peroneal perforator fasciocutaneous flaps; reconstruction of foot and ankle defects; reverse flow flaps; reverse peroneal artery flap.
Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures






Similar articles
-
Modified reversed superficial peroneal artery flap in the reconstruction of ankle and foot defects following severe burns or trauma.Burns. 2017 Jun;43(4):839-845. doi: 10.1016/j.burns.2016.12.003. Epub 2016 Dec 30. Burns. 2017. PMID: 28041753
-
Distally based perforator propeller sural flap for foot and ankle reconstruction: a modified flap dissection technique.Ann Plast Surg. 2014 Mar;72(3):340-5. doi: 10.1097/SAP.0b013e31826108f1. Ann Plast Surg. 2014. PMID: 23277108
-
Reconstruction of distal hand and foot defects with the free proximal peroneal artery perforator flap.Microsurgery. 2016 Mar;36(3):183-90. doi: 10.1002/micr.22364. Epub 2014 Dec 17. Microsurgery. 2016. PMID: 25516400
-
Peroneal artery perforator-based propeller flap reconstruction of the lateral distal lower extremity after tumor extirpation: case report and literature review.Microsurgery. 2008;28(8):663-70. doi: 10.1002/micr.20557. Microsurgery. 2008. PMID: 18846577 Review.
-
Distally based perforator flaps for reconstruction of post-traumatic defects of the lower leg and foot. A review of the anatomy and clinical outcomes.Injury. 2014 Mar;45(3):469-77. doi: 10.1016/j.injury.2013.09.003. Epub 2013 Sep 10. Injury. 2014. PMID: 24075220 Review.
References
-
- Godina M. Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg. 1986;78(03):285–292. - PubMed
-
- Follmar K E, Baccarani A, Baumeister S P, Levin L S, Erdmann D. The distally based sural flap. Plast Reconstr Surg. 2007;119(06):138e–148e. - PubMed
-
- Masquelet A C, Romana M C, Wolf G. Skin island flaps supplied by the vascular axis of the sensitive superficial nerves: anatomic study and clinical experience. Plast Reconstr Surg. 1992;89:1115–1121. - PubMed
-
- Masquelet A C, Beveridge J, Romana C, Gerber C. The lateral supramalleolar flap. Plast Reconstr Surg. 1988;81(01):74–81. - PubMed
LinkOut - more resources
Full Text Sources