

Combining local regional therapy and systemic therapy: Expected changes in the treatment landscape of recurrent hepatocellular carcinoma
- PMID: 36684055
- PMCID: PMC9850755
- DOI: 10.4251/wjgo.v15.i1.1
Combining local regional therapy and systemic therapy: Expected changes in the treatment landscape of recurrent hepatocellular carcinoma
Abstract
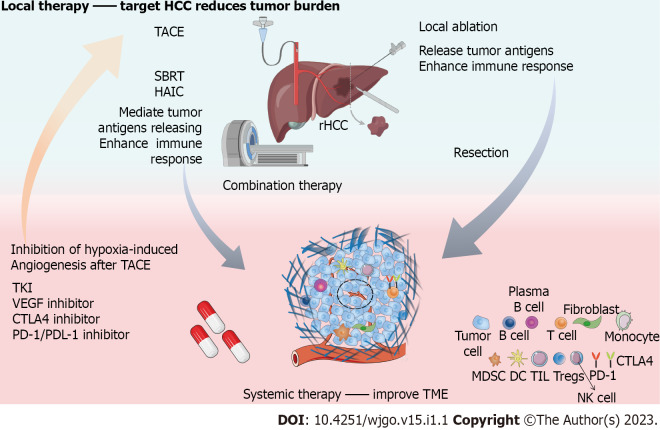
Improvements in early screening, new diagnostic techniques, and surgical treatment have led to continuous downward trends in hepatocellular carcinoma (HCC) morbidity and mortality rates. However, high recurrence and refractory cancer after hepatectomy remain important factors affecting the long-term prognosis of HCC. The clinical characteristics and prognosis of recurrent HCC are heterogeneous, and guidelines on treatment strategies for recurrent HCC are lacking. Therapies such as surgical resection, radiofrequency ablation, and transhepatic arterial chemoembolization are effective for tumors confined to the liver, and targeted therapy is a very important treatment for unresectable recurrent HCC with systemic metastasis. With the deepening of the understanding of the immune microenvironment of HCC, blocking immune checkpoints to enhance the antitumor immune response has become a new direction for the treatment of HCC. In addition, improvements in the tumor immune microenvironment caused by local treatment may provide an opportunity to improve the therapeutic effect of HCC treatment. Ongoing and future clinical trial data of combined therapy may develop the new treatment scheme for recurrent HCC. This paper reviews the pattern of recurrent HCC and the characteristics of the immune microenvironment, demonstrates the basis for combining local treatment and systemic treatment, and reports current evidence to better understand current progress and future approaches in the treatment of recurrent HCC.
Keywords: Immune checkpoint inhibitors; Local regional therapy; Recurrence type; Recurrent hepatocellular carcinoma; Systemic therapy; Tumor microenvironment.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures
Similar articles
-
Advancing precision medicine in hepatocellular carcinoma: current challenges and future directions in liquid biopsy, immune microenvironment, single nucleotide polymorphisms, and conversion therapy.Hepat Oncol. 2025 Dec;12(1):2493457. doi: 10.1080/20450923.2025.2493457. Epub 2025 Apr 22. Hepat Oncol. 2025. PMID: 40260687 Free PMC article. Review.
-
Strategies to Improve the Antitumor Effect of Immunotherapy for Hepatocellular Carcinoma.Front Immunol. 2021 Nov 26;12:783236. doi: 10.3389/fimmu.2021.783236. eCollection 2021. Front Immunol. 2021. PMID: 34899747 Free PMC article. Review.
-
Evolution of Systemic Treatment for Hepatocellular Carcinoma: Changing Treatment Strategies and Concepts.Cancers (Basel). 2024 Jun 28;16(13):2387. doi: 10.3390/cancers16132387. Cancers (Basel). 2024. PMID: 39001448 Free PMC article. Review.
-
The 10-year Survival Analysis of Radiofrequency Ablation for Solitary Hepatocellular Carcinoma 5 cm or Smaller: Primary versus Recurrent HCC.Radiology. 2021 Aug;300(2):458-469. doi: 10.1148/radiol.2021200153. Epub 2021 May 18. Radiology. 2021. PMID: 34003058
-
Conversion surgery after preoperative therapy for advanced hepatocellular carcinoma in the era of molecular targeted therapy and immune checkpoint inhibitors.J Hepatobiliary Pancreat Sci. 2022 Jul;29(7):732-740. doi: 10.1002/jhbp.1135. Epub 2022 Mar 31. J Hepatobiliary Pancreat Sci. 2022. PMID: 35306748 Review.
Cited by
-
Combination therapy strategy based on selective internal radiation therapy as conversion therapy for inoperable giant hepatocellular carcinoma: A case report.World J Gastrointest Oncol. 2025 Mar 15;17(3):100861. doi: 10.4251/wjgo.v17.i3.100861. World J Gastrointest Oncol. 2025. PMID: 40092927 Free PMC article.
-
Transarterial chemoembolization with molecular targeted therapies plus camrelizumab for recurrent hepatocellular carcinoma.BMC Cancer. 2024 Mar 27;24(1):387. doi: 10.1186/s12885-024-12144-6. BMC Cancer. 2024. PMID: 38539150 Free PMC article.
-
Effect of regorafenib combined with immunotherapy and arterial chemoembolization on the survival of patients with advanced hepatocellular carcinoma: a retrospective study.Am J Transl Res. 2025 Mar 15;17(3):1962-1973. doi: 10.62347/BXYO6569. eCollection 2025. Am J Transl Res. 2025. PMID: 40226031 Free PMC article.
-
Navigating the complexities: challenges and opportunities in conversion therapy for advanced hepatocellular carcinoma.Clin Exp Med. 2025 May 18;25(1):169. doi: 10.1007/s10238-025-01698-9. Clin Exp Med. 2025. PMID: 40382739 Free PMC article. Review.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261:947–955. - PubMed
-
- Shah SA, Cleary SP, Wei AC, Yang I, Taylor BR, Hemming AW, Langer B, Grant DR, Greig PD, Gallinger S. Recurrence after liver resection for hepatocellular carcinoma: risk factors, treatment, and outcomes. Surgery. 2007;141:330–339. - PubMed
-
- European Association for the Study of the Liver ; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
