

Double-stapled anastomosis without "dog-ears" reduces the anastomotic leakage in laparoscopic anterior resection of rectal cancer: A prospective, randomized, controlled study
- PMID: 36684218
- PMCID: PMC9852307
- DOI: 10.3389/fsurg.2022.1003854
Double-stapled anastomosis without "dog-ears" reduces the anastomotic leakage in laparoscopic anterior resection of rectal cancer: A prospective, randomized, controlled study
Abstract
Background: Anastomotic leakage (AL) is a major cause of postoperative morbidity and mortality in the treatment of colorectal cancer. The aim of this study was to investigate whether the resection of "dog-ears" in laparoscopic anterior resection of rectal cancer (called modified double-stapling technique, MDST) could reduce the rate of AL in patients with middle and high rectal cancer, as compared with the conventional double-stapling technique (DST).
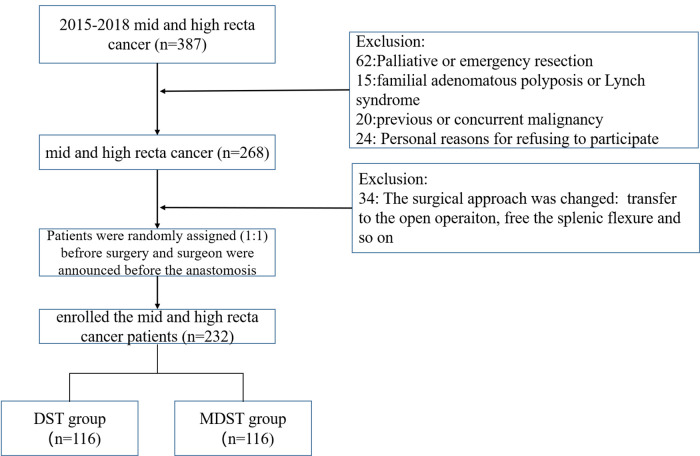
Methods: The clinical data of 232 patients with middle and high rectal cancer were prospectively collected from September 2015 to October 2018. They were randomly divided into the MDST group (n = 116) and the DST group (n = 116) and the data were prospectively analyzed. Morbidity and AL rate were compared between the two groups.
Results: Patient demographics, tumor size, and time of first flatus were similar between the two groups. No difference was observed in the operation time between the two groups. The AL rate was significantly lower in the MDST group than in the DST group (3.4 vs. 11.2%, p = 0.032). The age and anastomotic technique were the factors associated with AL according to the multivariate analysis. The location of the AL in the DST group was further investigated, revealing that AL was in the same place as the "dog-ears" (11/13, 84.6%).
Conclusions: Our prospective comparative study demonstrated that MDST have a better short-term outcome in reducing AL compared with DST. Therefore, this technique could be an alternative approach to maximize the benefit of laparoscopic anterior resection on patients with middle and high rectal cancer. The "dog-ears" create stapled corners potentially ischemic, since they represent the area with high incidence of AL.(NCT:02770911).
Keywords: anastomotic leakage; anterior resection; laparoscopic; middle and high rectal cancer; modified double-stapling technique.
© 2023 Yang, Ding, Xu, Pan, Zhuang, Liu and Guan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. (2005) 365:1718–26. 10.1016/S0140-6736(05)66545-2 - DOI - PubMed
-
- Jeong SY, Park JW, Nam BH, Kim S, Kang SB, Lim SB, et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. (2014) 15:767–74. 10.1016/S1470-2045(14)70205-0 - DOI - PubMed
LinkOut - more resources
Full Text Sources