

Novel end-to-side one-layer continuous pancreaticojejunostomy vs. end-to-end invaginated pancreaticojejunostomy in pancreatoduodenectomy: A single-center retrospective study
- PMID: 36684316
- PMCID: PMC9852522
- DOI: 10.3389/fsurg.2022.980056
Novel end-to-side one-layer continuous pancreaticojejunostomy vs. end-to-end invaginated pancreaticojejunostomy in pancreatoduodenectomy: A single-center retrospective study
Abstract
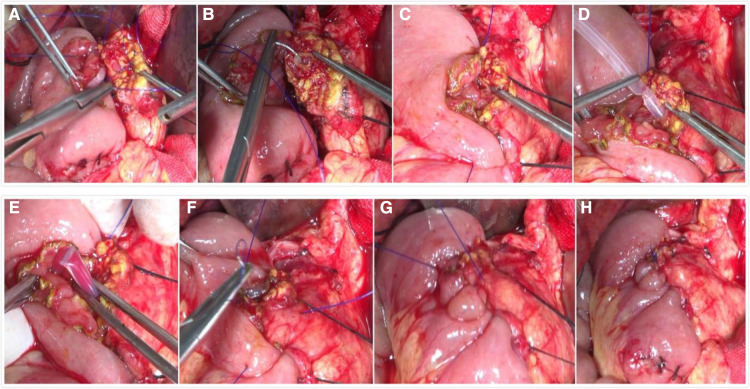
Background and objective: Postoperative pancreatic fistula (POPF) is the most common critical complication after pancreatoduodenectomy (PD) and is the primary reason for increased mortality and morbidity after PD. We aim to investigate the clinical significance of a novel approach, i.e., end-to-side one-layer continuous pancreaticojejunostomy, for patients with PD.
Methods: The clinical data of 65 patients who underwent pancreatoduodenectomy at the Xiangya Hospital, Central South University, from September 2020 to December 2021 were retrospectively analyzed.
Results: Forty patients underwent end-to-end invaginated pancreaticojejunostomy, and 25 underwent the novel end-to-side one-layer continuous pancreaticojejunostomy. No significant differences were observed in pancreatic fistula, intraperitoneal infection, intraperitoneal bleeding, reoperation, postoperative hospital stay, or perioperative death between the two groups. However, the novel end-to-side one-layer continuous pancreaticojejunostomy group had significantly shorter operation duration (32.6 ± 5.1 min vs. 8.3 ± 2.2 min, p < 0.001). The incidence of pancreatic fistula in the novel pancreaticojejunostomy group was 12%, including two cases of grade A POPF and only one case of grade B POPF. No cases of grade C POPF occurred. No deaths were observed during the perioperative period.
Conclusions: The novel anastomosis method leads to a shorter operation duration than the traditional anastomosis method and does not increase postoperative complications. In conclusion, it is a simplified and feasible method for pancreatic anastomosis.
Keywords: end-to-side pancreaticojejunostomy; one-layer continuous pancreaticojejunostomy; pancreatic anastomosis; pancreatic fistula; pancreaticoduodenectomy.
© 2023 Luo, Li, Ji and Gong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effect of Blumgart anastomosis in reducing the incidence rate of pancreatic fistula after pancreatoduodenectomy.World J Gastroenterol. 2019 May 28;25(20):2514-2523. doi: 10.3748/wjg.v25.i20.2514. World J Gastroenterol. 2019. PMID: 31171894 Free PMC article.
-
Clinical evaluation of modified invaginated pancreaticojejunostomy for pancreaticoduodenectomy.World J Surg Oncol. 2020 Apr 15;18(1):75. doi: 10.1186/s12957-020-01851-6. World J Surg Oncol. 2020. PMID: 32295594 Free PMC article.
-
Pancreaticojejunostomy with double-layer continuous suturing is associated with a lower risk of pancreatic fistula after pancreaticoduodenectomy: a comparative study.Int J Surg. 2015 Jan;13:84-89. doi: 10.1016/j.ijsu.2014.11.034. Epub 2014 Dec 4. Int J Surg. 2015. PMID: 25481836
-
A web-based overview, systematic review and meta-analysis of pancreatic anastomosis techniques following pancreatoduodenectomy.HPB (Oxford). 2018 Sep;20(9):777-785. doi: 10.1016/j.hpb.2018.03.003. HPB (Oxford). 2018. PMID: 29773356
-
Stent A pancreaticojejunostomy after pancreatoduodenectomy: Is it always necessary?World J Methodol. 2024 Sep 20;14(3):90164. doi: 10.5662/wjm.v14.i3.90164. eCollection 2024 Sep 20. World J Methodol. 2024. PMID: 39310242 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources