

Management of hemodynamically stable wide QRS complex tachycardia in patients with implantable cardioverter defibrillators
- PMID: 36684577
- PMCID: PMC9846131
- DOI: 10.3389/fcvm.2022.1011619
Management of hemodynamically stable wide QRS complex tachycardia in patients with implantable cardioverter defibrillators
Abstract
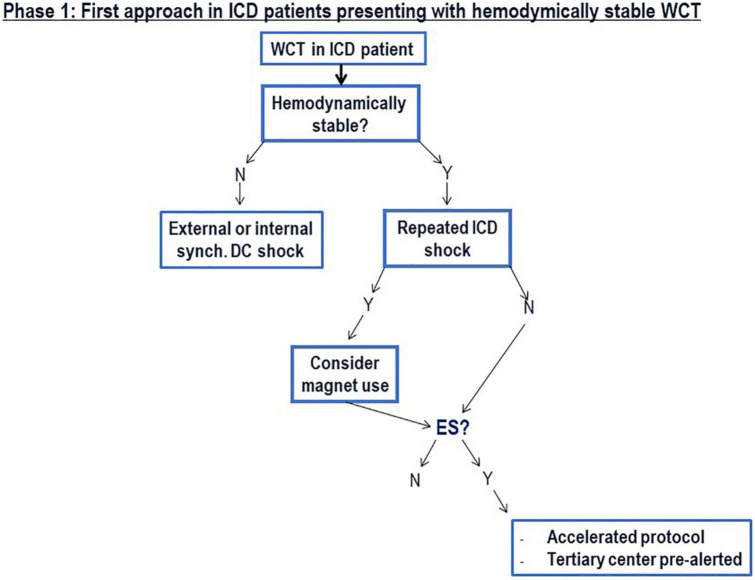
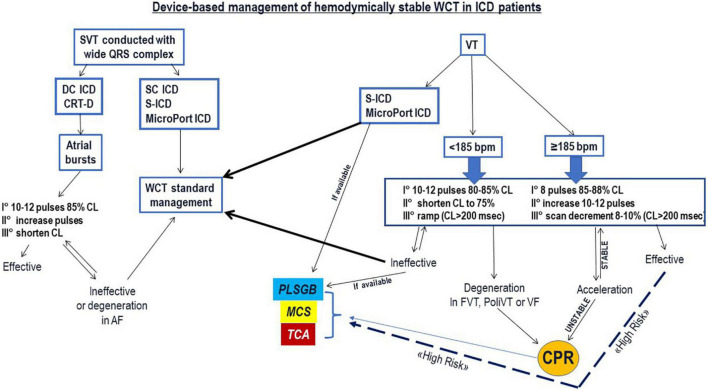
Management of hemodynamically stable, incessant wide QRS complex tachycardia (WCT) in patients who already have an implantable cardioverter defibrillator (ICD) is challenging. First-line treatment is performed by medical staff who have no knowledge on programmed ICD therapy settings and there is always some concern for unexpected ICD shock. In these patients, a structured approach is necessary from presentation to therapy. The present review provides a systematic approach in four distinct phases to guide any physician involved in the management of these patients: PHASE I: assessment of hemodynamic status and use of the magnet to temporarily suspend ICD therapies, especially shocks; identification of possible arrhythmia triggers; risk stratification in case of electrical storm (ES).
Phase ii: The preparation phase includes reversal of potential arrhythmia "triggers", mild patient sedation, and patient monitoring for therapy delivery. Based on resource availability and competences, the most adequate therapeutic approach is chosen. This choice depends on whether a device specialist is readily available or not. In the case of ES in a "high-risk" patient an accelerated patient management protocol is advocated, which considers urgent ventricular tachycardia transcatheter ablation with or without mechanical cardiocirculatory support.
Phase iii: Therapeutic phase is based on the use of intravenous anti-arrhythmic drugs mostly indicated in this clinical context are presented. Device interrogation is very important in this phase when sustained monomorphic VT diagnosis is confirmed, then ICD ATP algorithms, based on underlying VT cycle length, are proposed. In high-risk patients with intractable ES, intensive patient management considers MCS and transcatheter ablation.
Phase iv: The patient is hospitalized for further diagnostics and management aimed at preventing arrhythmia recurrences.
Keywords: ICD programming; ICD therapies; anti-tachycardia pacing; treatment of ventricular tachycardia; wide QRS complex tachycardia.
Copyright © 2023 Regoli, Cattaneo, Kola, Thartori, Bytyci, Saccarello, Amoruso, Di Valentino and Menafoglio.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Ventricular Tachycardia with ICD Shocks: When to Medicate and When to Ablate.Curr Cardiol Rep. 2017 Sep 13;19(11):105. doi: 10.1007/s11886-017-0924-0. Curr Cardiol Rep. 2017. PMID: 28900864 Review.
-
Implantable cardioverter-defibrillator programming and electrical storm: Results of the OBSERVational registry On long-term outcome of ICD patients (OBSERVO-ICD).Heart Rhythm. 2016 Oct;13(10):1987-92. doi: 10.1016/j.hrthm.2016.06.007. Epub 2016 Jun 9. Heart Rhythm. 2016. PMID: 27291511
-
Outcomes of defibrillator therapy in catecholaminergic polymorphic ventricular tachycardia.Heart Rhythm. 2014 Jan;11(1):58-66. doi: 10.1016/j.hrthm.2013.10.027. Epub 2013 Oct 11. Heart Rhythm. 2014. PMID: 24120999
-
Case report: Short-long-short mechanism triggering sustained ventricular tachycardia in a patient with a single-chamber ICD but inhibiting antitachycardia therapy.Front Cardiovasc Med. 2022 Aug 26;9:984262. doi: 10.3389/fcvm.2022.984262. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36093158 Free PMC article.
-
Electrical storm: A clinical and electrophysiological overview.World J Cardiol. 2015 Sep 26;7(9):555-61. doi: 10.4330/wjc.v7.i9.555. World J Cardiol. 2015. PMID: 26413232 Free PMC article. Review.
Cited by
-
Artificial Intelligence and Heart-Brain Connections: A Narrative Review on Algorithms Utilization in Clinical Practice.Healthcare (Basel). 2024 Jul 10;12(14):1380. doi: 10.3390/healthcare12141380. Healthcare (Basel). 2024. PMID: 39057522 Free PMC article. Review.
References
-
- Schaer B, Kühne M, Reichlin T, Osswald S, Sticherling C. Incidence of and predictors for appropriate implantable cardioverter-defibrillator therapy in patients with a secondary preventive implantable cardioverter-defibrillator indication. Europace. (2016) 18:227–31. 10.1093/europace/euv188 - DOI - PubMed
-
- Zaman S, Sivagangabalan G, Chik W, Stafford W, Hayes J, Denman R, et al. Ventricular tachyarrhythmia recurrence in primary versus secondary implantable cardioverter-defibrillator patients and role of electrophysiology study. J Interv Card Electrophysiol. (2014) 41:195–202. 10.1007/s10840-014-9941-8 - DOI - PubMed
-
- Brugada J, Katritsis D, Arbelo E, Arribas F, Bax J, Blomström-Lundqvist C, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardia. The task force for the management of patients with supraventricular tachycardia of the European society of cardiology (ESC). Eur Heart J. (2021) 41:655–720. - PubMed
-
- Deyell M, AbdelWahab A, Angaran P, Essebag V, Glover B, Gula L, et al. Members of the secondary panel. 2020 Canadian cardiovascular society/Canadian heart rhythm society position statement on the management of ventricular tachycardia and fibrillation in patients with structural heart disease. Can J Cardiol. (2020) 36:822–36. 10.1016/j.cjca.2020.04.004 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources