

How to interpret serum creatinine increases during decongestion
- PMID: 36684603
- PMCID: PMC9846337
- DOI: 10.3389/fcvm.2022.1098553
How to interpret serum creatinine increases during decongestion
Abstract
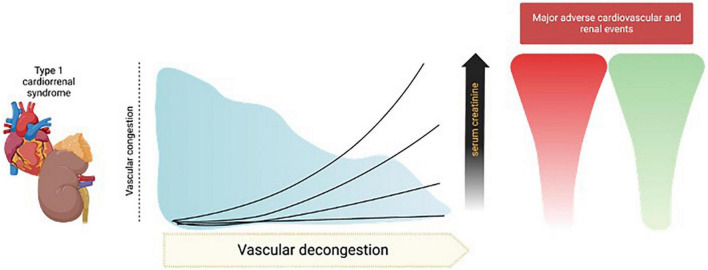
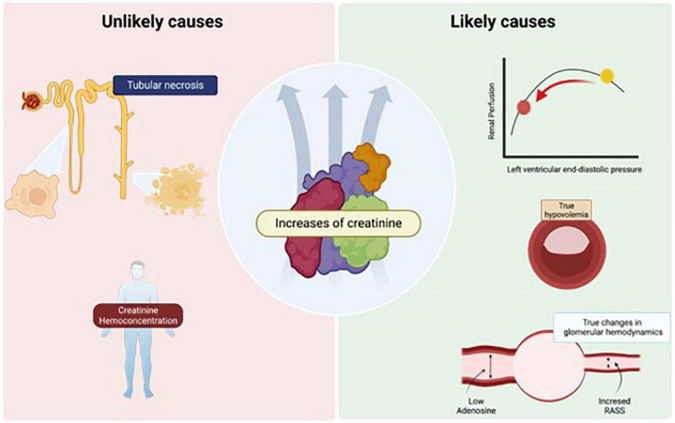
During decongestion in acute decompensated heart failure (ADHF), it is common to observe elevations in serum creatinine (sCr) values due to vascular congestion, a mechanism that involves increased central venous pressure that has a negative impact on the nephron, promoting greater absorption of water and sodium, increased interstitial pressure in an encapsulated organ developing "renal tamponade" which is one of main physiopathological mechanism associated with impaired kidney function. For the treatment of this syndrome, it is recommended to use diuretics that generate a high urinary output and natriuresis to decongest the venous system, during this process the sCr values can rise, a phenomenon that may bother some cardiologist and nephrologist, since raise the suspicion of kidney damage that could worsen the prognosis of these patients. It is recommended that increases of up to 0.5 mg/dL from baseline are acceptable, but some patients have higher increases, and we believe that an arbitrary number would be impractical for everyone. These increases in sCr may be related to changes in glomerular hemodynamics and true hypovolemia associated with decongestion, but it is unlikely that they are due to structural injury or truly hypoperfusion and may even have a positive connotation if accompanied by an effective decongestion and be associated with a better prognosis in the medium to long term with fewer major cardiovascular and renal events. In this review, we give a comprehensive point of view on the interpretation of creatinine elevation during decongestion in patients with ADHF.
Keywords: AKI; acute heart failure; cardiorenal syndrome 1; creatinine; decongestion.
Copyright © 2023 Chávez-Íñiguez, Ivey-Miranda, De la Vega-Mendez and Borges-Vela.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources