

Impact of Pre-Existing Ischemic Heart Disease on Severe Maternal Morbidity and Mortality During Delivery Hospitalizations
- PMID: 36684662
- PMCID: PMC9851052
- DOI: 10.1016/j.jacadv.2022.100157
Impact of Pre-Existing Ischemic Heart Disease on Severe Maternal Morbidity and Mortality During Delivery Hospitalizations
Abstract
Background: The impact of pre-existing ischemic heart disease (IHD) on pregnancy is incompletely described.
Objectives: The purpose of this study was to compare adverse pregnancy outcomes between those with IHD and those with a cardiac diagnosis categorized by the modified World Health Organization classification and those without a cardiac diagnosis.
Methods: This retrospective study used the 2015 to 2018 Nationwide Readmissions Database. Delivery hospitalizations, comorbidities, and outcomes were identified using diagnosis and procedure codes. The exposure was isolated IHD. The primary outcome was severe maternal morbidity (SMM) or death during the delivery hospitalization, analyzed using adjusted relative risk (aRR) regression and weighted to account for the Nationwide Readmissions Database's complex survey methods.
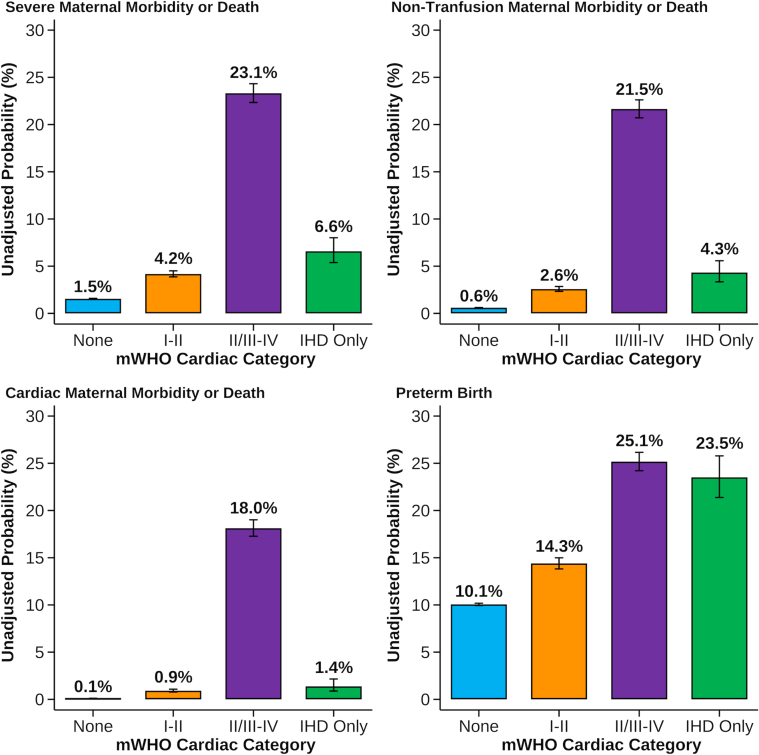
Results: Of 11,556,136 delivery hospitalizations, 65,331 had another cardiac diagnosis, and 3,009 had IHD alone. Patients with IHD were older and had higher rates of diabetes and hypertension. In unadjusted analyses, adverse outcomes were more common among patients with IHD alone than among patients with no cardiac disease and modified World Health Organization class I-II disease. After adjustment, patients with IHD alone were associated with a higher risk of SMM or death (aRR: 1.51; 95% CI: 1.19-1.92) than those without a cardiac disease. In comparison, the aRR was 1.90 (95% CI: 1.76-2.06) for WHO class I-II diseases and 5.87 (95% CI: 5.49-6.27) for WHO II/III-IV diseases. Nontransfusion SMM or death (aRR: 1.60; 95% CI: 1.11-2.30) and cardiac SMM or death (aRR: 2.98; 95% CI: 1.75-5.08) were also higher for those with IHD.
Conclusions: Isolated IHD in pregnancy is associated with worse outcomes than no cardiac disease during delivery hospitalization and approximates the risk associated with WHO I-II diagnoses.
Keywords: coronary artery disease; ischemic heart disease; maternal mortality; modified World Health Organization classification; severe maternal morbidity.
Conflict of interest statement
The work reported in this paper was made possible by the following grants from the National Institutes of Health: TL1-TR002555 (to Dr Federspiel). Data acquisition was also supported by funding from the Foundation for Women and Girls with Blood Disorders to Dr Federspiel. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



Comment in
-
When Burdened by Ischemic Heart Disease, Pregnant Individuals Lose the Advantage of Youth.JACC Adv. 2022 Dec 30;1(5):100159. doi: 10.1016/j.jacadv.2022.100159. eCollection 2022 Dec. JACC Adv. 2022. PMID: 38939470 Free PMC article.
References
-
- Martin J.A., Hamilton B.E., Osterman M.J.K., Driscoll A.K. Births: final data for 2019. Natl Vital Stat Rep. 2021;70:1–51. - PubMed
-
- James A.H., Jamison M.G., Biswas M.S., Brancazio L.R., Swamy G.K., Myers E.R. Acute myocardial infarction in pregnancy: a United States population-based study. Circulation. 2006;113:1564–1571. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
