

An Updated Approach to Antiobesity Pharmacotherapy: Moving Beyond the 5% Weight Loss Goal
- PMID: 36686585
- PMCID: PMC9847544
- DOI: 10.1210/jendso/bvac195
An Updated Approach to Antiobesity Pharmacotherapy: Moving Beyond the 5% Weight Loss Goal
Abstract
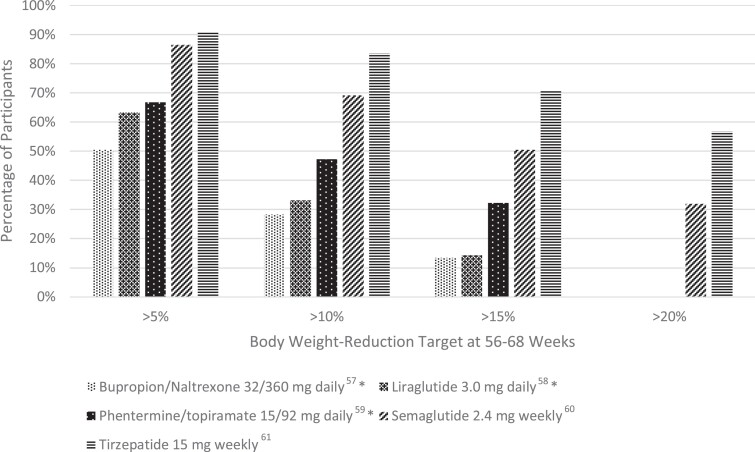
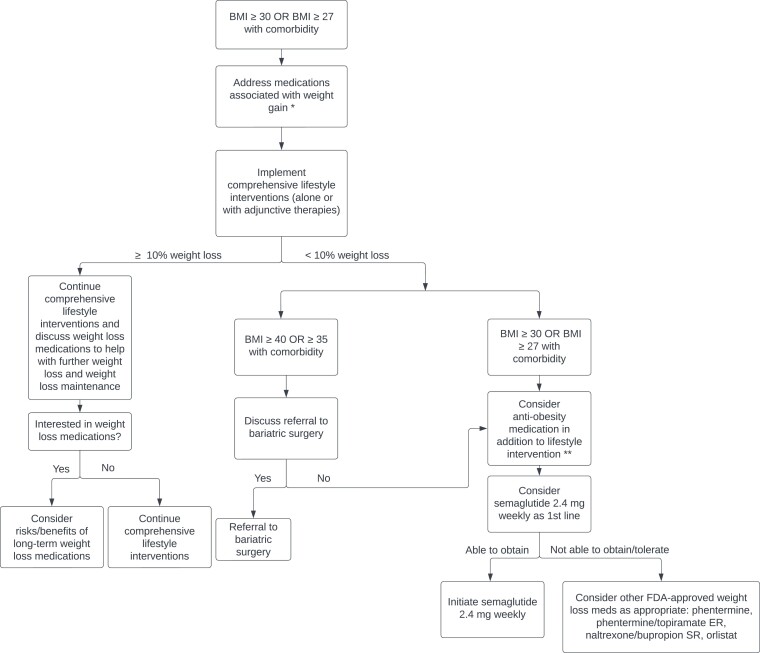
Despite professional society guidelines recommending that obesity be treated as a chronic disease by emphasizing the use of lifestyle modification in conjunction with pharmacotherapy, antiobesity medications are uncommonly prescribed in most clinical practices. The recent Food and Drug Administration approval of semaglutide 2.4 mg weekly to treat obesity-as well as other forthcoming advancements in diabetes and antiobesity medications-highlights the potential of pharmacotherapy to significantly augment weight loss efforts. In this Expert Endocrine Consult, we review the evolving role of antiobesity pharmacotherapy in clinical practice and suggest a framework for the use of these medications.
Keywords: antiobesity pharmacotherapy; obesity; weight loss.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Ward ZJ, Bleich SN, Cradock AL, et al. Projected U.S. state-level prevalence of adult obesity and severe obesity. N Engl J Med. 2019;381(25):2440–2450. - PubMed
-
- Jiang L, Rong J, Wang Y, et al. The relationship between body mass index and hip osteoarthritis: a systematic review and meta-analysis. Joint Bone Spine. 2011;78(2):150–155. - PubMed
Publication types
LinkOut - more resources
Full Text Sources