

MRI-based multiregional radiomics for predicting lymph nodes status and prognosis in patients with resectable rectal cancer
- PMID: 36686763
- PMCID: PMC9846353
- DOI: 10.3389/fonc.2022.1087882
MRI-based multiregional radiomics for predicting lymph nodes status and prognosis in patients with resectable rectal cancer
Abstract
Purpose: To establish and evaluate multiregional T2-weighted imaging (T2WI)-based clinical-radiomics model for predicting lymph node metastasis (LNM) and prognosis in patients with resectable rectal cancer.
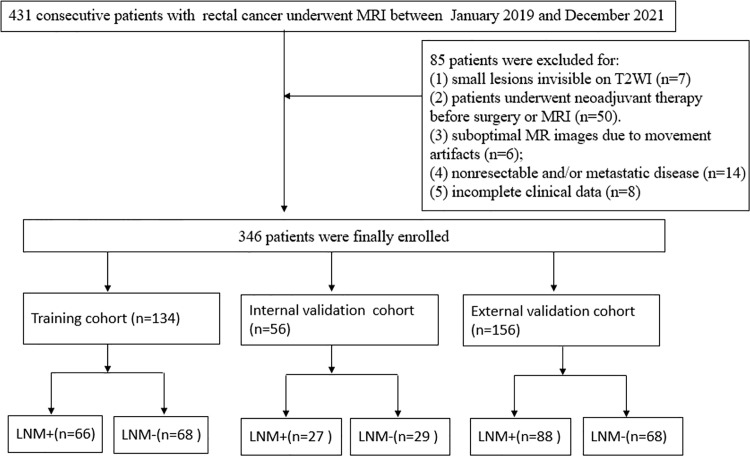
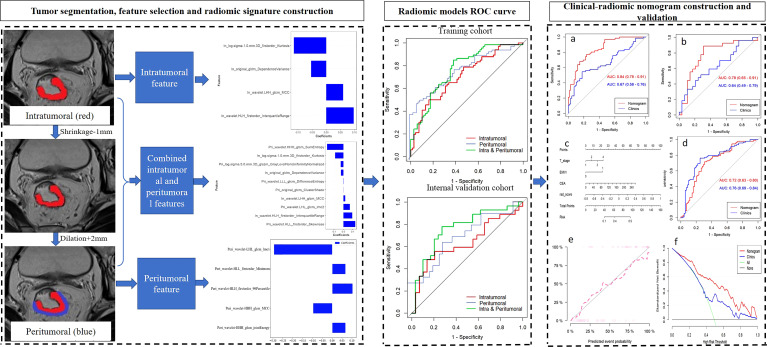
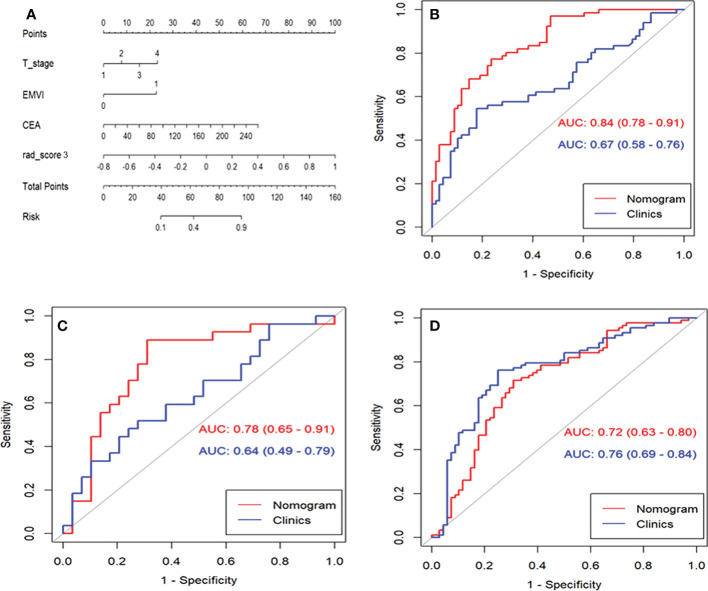
Methods: A total of 346 patients with pathologically confirmed rectal cancer from two hospitals between January 2019 and December 2021 were prospectively enrolled. Intra- and peritumoral features were extracted separately, and least absolute shrinkage and selection operator regression was applied for feature selection. Radiomics signatures were built using the selected features from different regions. The clinical-radiomic nomogram was developed by combining the intratumoral and peritumoral radiomics signatures score (radscore) and the most predictive clinical parameters. The diagnostic performances of the nomogram and clinical model were evaluated using the area under the receiver operating characteristic curve (AUC). The prognostic model for 3-year recurrence-free survival (RFS) was constructed using univariate and multivariate Cox analysis.
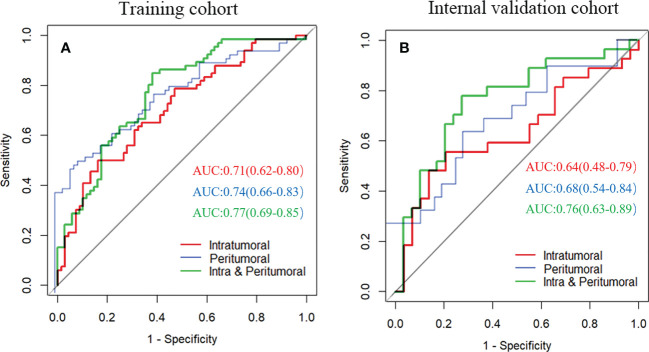
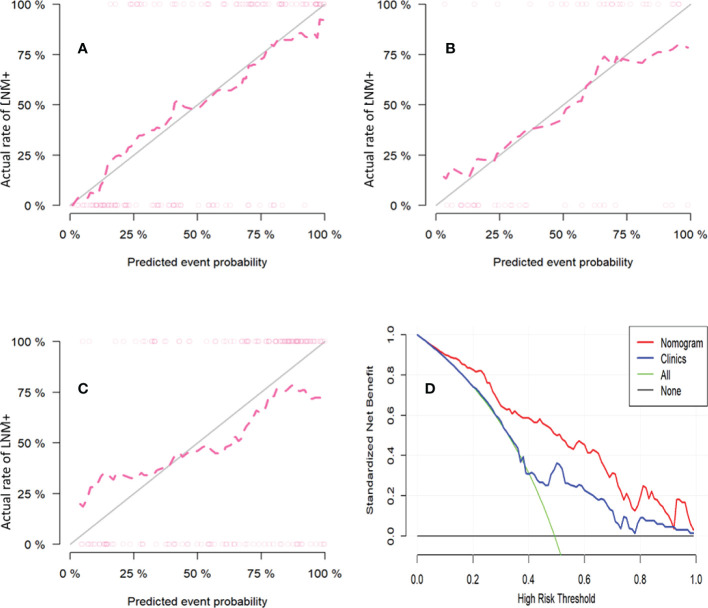
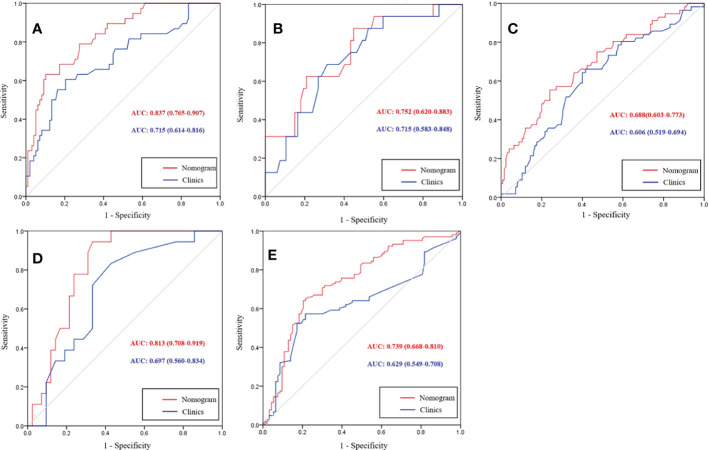
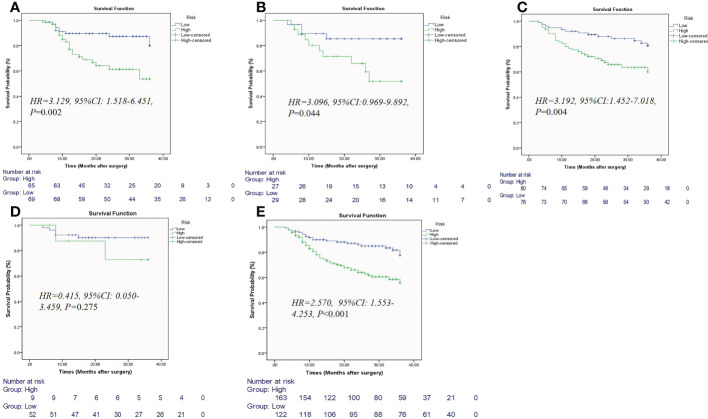
Results: The intratumoral radscore (radscore 1) included four features, the peritumoral radscore (radscore 2) included five features, and the combined intratumoral and peritumoural radscore (radscore 3) included ten features. The AUCs for radscore 3 were higher than that of radscore 1 in training cohort (0.77 vs. 0.71, P=0.182) and internal validation cohort (0.76 vs. 0.64, P=0.041). The AUCs for radscore 3 were higher than that of radscore 2 in training cohort (0.77 vs. 0.74, P=0.215) and internal validation cohort (0.76 vs. 0.68, P=0.083). A clinical-radiomic nomogram showed a higher AUC compared with the clinical model in training cohort (0.84 vs. 0.67, P<0.001) and internal validation cohort (0.78 vs. 0.64, P=0.038) but not in external validation (0.72 vs. 0.76, P=0.164). Multivariate Cox analysis showed MRI-reported extramural vascular invasion (EMVI) (HR=1.099, 95%CI: 0.462-2.616; P=0.031) and clinical-radiomic nomogram-based LNM (HR=2.232, 95%CI:1.238-7.439; P=0.017) were independent risk factors for assessing 3-year RFS. Combined clinical-radiomic nomogram based LNM and MRI-reported EMVI showed good performance in training cohort (AUC=0.748), internal validation cohort (AUC=0.706) and external validation (AUC=0.688) for predicting 3-year RFS.
Conclusion: A clinical-radiomics nomogram exhibits good performance for predicting preoperative LNM. Combined clinical-radiomic nomogram based LNM and MRI-reported EMVI showed clinical potential for assessing 3-year RFS.
Keywords: lymph node; magnetic resonance imaging; prognosis; radiomics; rectal neoplasms.
Copyright © 2023 Li, Chen, Liu, Lu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources