

Closure strategy for endoscopic pituitary surgery: Experience from 3015 patients
- PMID: 36686774
- PMCID: PMC9846073
- DOI: 10.3389/fonc.2022.1067312
Closure strategy for endoscopic pituitary surgery: Experience from 3015 patients
Abstract
Introduction: Effective strategies are required to ensure optimal management of the crucial closure step in endoscopic pituitary surgery. Many surgical techniques have been reported but no significant consensus has been defined.
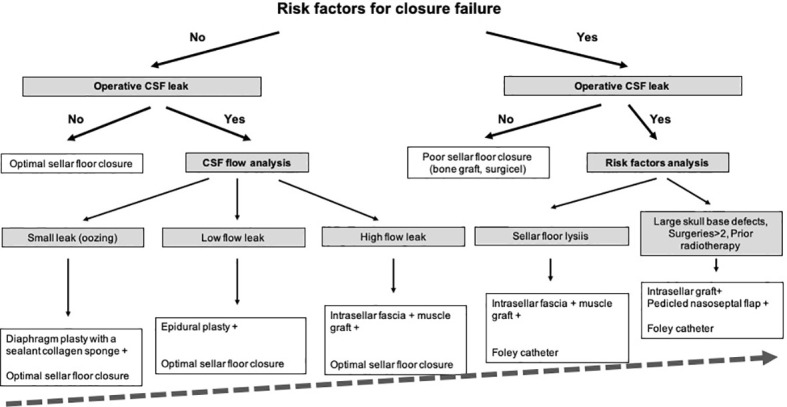
Methods: Between January 2006 and March 2022, 3015 adult patients with pituitary adenomas were operated on by a single expert neurosurgical team, using a mononostril endoscopic endonasal approach. Based of preoperative risk factors of and operative findings, a detailed closure strategy was used. Body mass index >40, sellar floor lysis, number of surgeries>2, large skull base destruction, prior radiotherapy were considered as preoperative risk factors for closure failure. All patients treated with an expanded endonasal approach were excluded.
Results: Patients were mostly women (F/M ratio: 1.4) with a median age of 50 (range: 18 -89). Intraoperative CSF leak requiring specific surgical management was observed in 319/3015 (10.6%) of patients. If intraoperative leak occurred, patients with predictive risk factors were managed using a Foley balloon catheter in case of sellar floor lysis or BMI>40 and a multilayer repair strategy with a vascularized nasoseptal flap in other cases. Postoperative CSF leak occurred in 29/3015 (1%) of patients, while meningitis occurred in 24/3015 (0.8%) of patients. In patients with intraoperative leak, closure management failed in 11/319 (3.4%) of cases.
Conclusion: Based on our significant 16-year experience, our surgical management is reliable and easy to follow. With a planned and stepwise strategy, the closure step can be optimized and tailored to each patient with a very low failure rate.
Keywords: closure; endoscopy; nasoseptal flap; pituitary surgery; skull base repair; strategy.
Copyright © 2023 Baussart, Venier, Jouinot, Reuter and Gaillard.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources