

Endoplasmic reticulum stress related IncRNA signature predicts the prognosis and immune response evaluation of uterine corpus endometrial carcinoma
- PMID: 36686816
- PMCID: PMC9848491
- DOI: 10.3389/fonc.2022.1064223
Endoplasmic reticulum stress related IncRNA signature predicts the prognosis and immune response evaluation of uterine corpus endometrial carcinoma
Abstract
Background: Endoplasmic reticulum (ER) stress is closely related to the occurrence, development and treatment of tumors. Recent studies suggest ER stress as a therapeutic strategy of choice for cancer. However, ER stress-related long non-coding RNA (lncRNA) predictive value in endometrial carcinoma (UCEC) remains to be further evaluated. The purpose of this study was to establish relies on the signature of ER stress-related lncRNA forecast to predict the prognosis of patients with UCEC.
Methods: We downloaded the RNA expression profile dataset and matched clinical data from the Cancer Genome Atlas (TCGA) database, and applied univariate and multivariate Cox regression analysis to build predictive signature. Kaplan-meier method was used to evaluate overall survival (OS) and disease-free survival (DFS). Gene set enrichment analysis (GSEA) was used to study the functional characteristics. Single sample Gene set enrichment analysis (ssGSEA) was used to analyze the relationship between immune status and predicted signature. Correlations between the potential usefulness of treatment for UCEC patients and predictive signature were also analyzed.
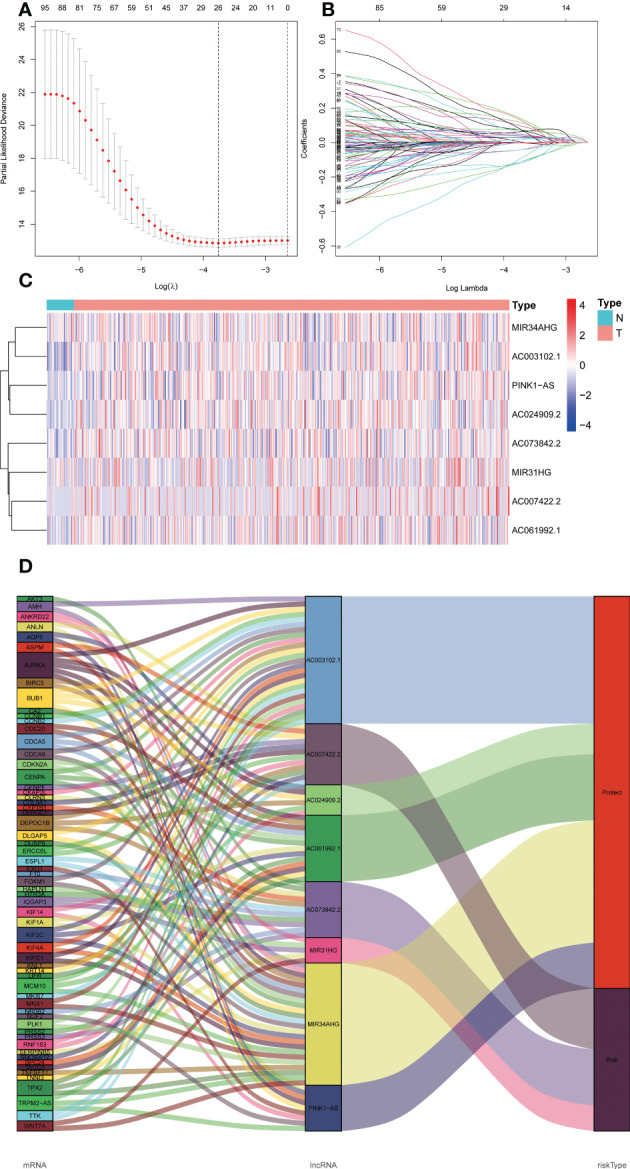
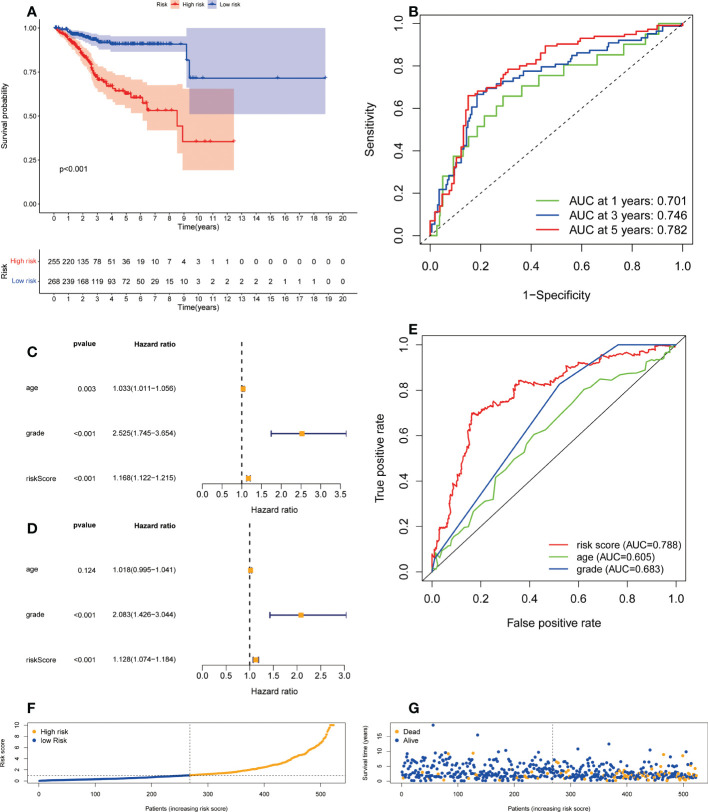
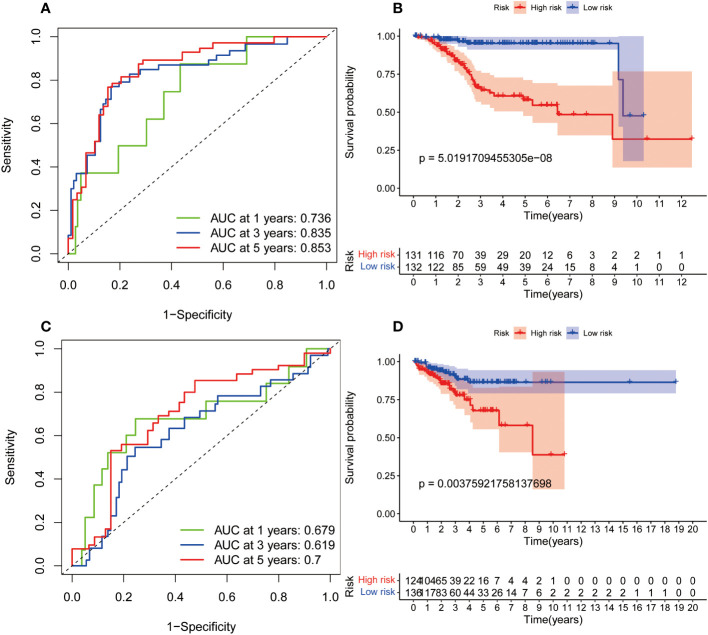
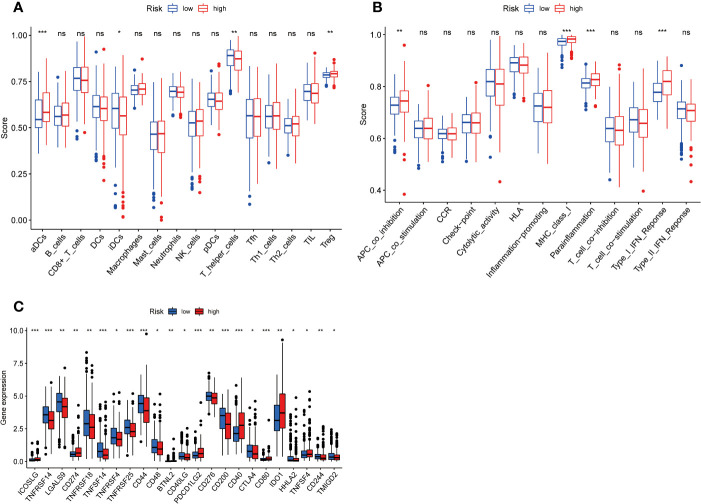
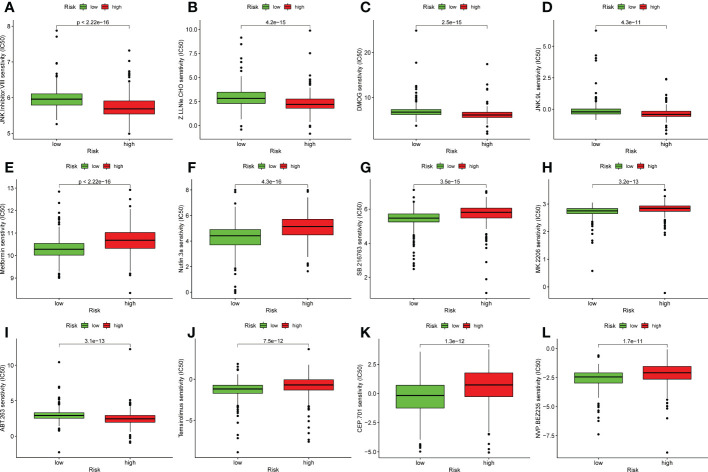
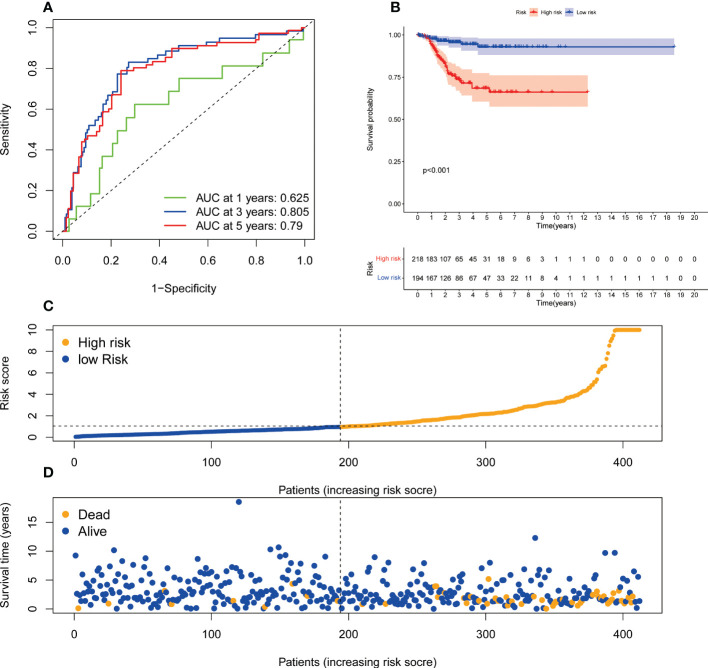
Results: We established a signature composed of eight ER stress-related lncRNAs (MIR34AHG, AC073842.2, PINK1AS, AC024909.2, MIR31HG, AC007422.2, AC061992.1, AC003102.1). The signature of ER stress-related lncRNA provided better diagnostic value compared with age and tumor grade, and the area under the receiver operating curve was 0.788. The overall and disease-free survival probability of patients in the high-risk group is lower than that in the low-risk group. GSEA indicated that the pathways were mainly enriched for cancer, immunity and reproduction related pathways. ss-GSEA shows that prediction signature and activation of dendritic cells, immature dendritic cells, T helper cells and immune status of the Treg are significantly related. High-risk groups may against PD - 1/L1 immunotherapy and JNK inhibitors VIII, Z.LLNle.CHO, DMOG and JNK. 9 l more sensitive.
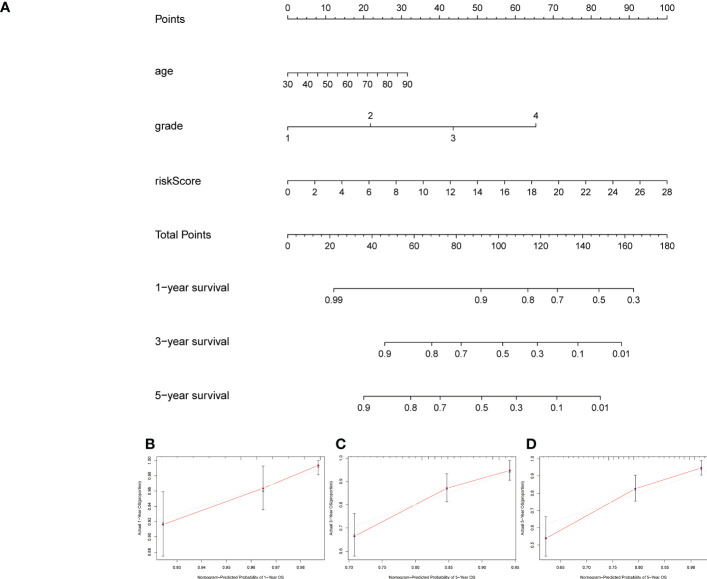
Conclusion: The ER stress signature can independently predict the prognosis of UCEC patients, and provide guidance for conventional chemotherapy and immunotherapy of UCEC patients.
Keywords: ER stress; drug therapy; immune infiltration; lncRNAs; uterine corpus endometrial carcinoma.
Copyright © 2023 Chen, Shen and Yang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Liu J, Yin J, Wang Y, Cai L, Geng R, Du M, et al. A comprehensive prognostic and immune analysis of enhancer RNA identifies IGFBP7-AS1 as a novel prognostic biomarker in uterine corpus endometrial carcinoma. Biol Procedures Online. (2022) 24(1):9. doi: 10.1186/s12575-022-00172-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials