

Case Report: Pituitary metastasis as a presenting manifestation of silent gastric cardia adenocarcinoma
- PMID: 36686817
- PMCID: PMC9846627
- DOI: 10.3389/fonc.2022.1059361
Case Report: Pituitary metastasis as a presenting manifestation of silent gastric cardia adenocarcinoma
Abstract
Introduction: Pituitary metastases are very rare in cancer patients and often originate from lung or breast tumors. They usually occur in patients with known metastatic disease, but rarely may be the first presentation of the primary tumor.
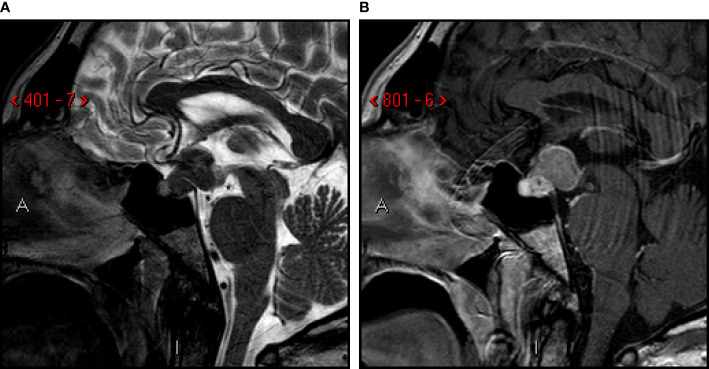
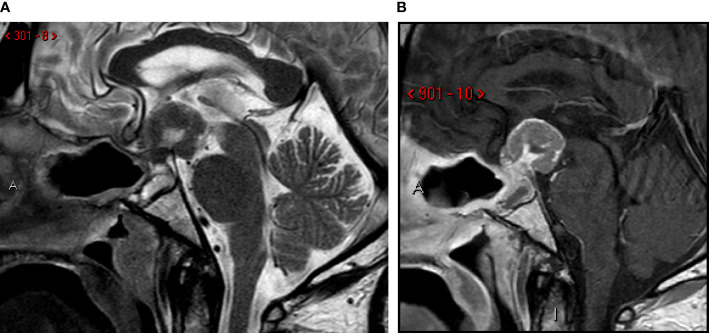
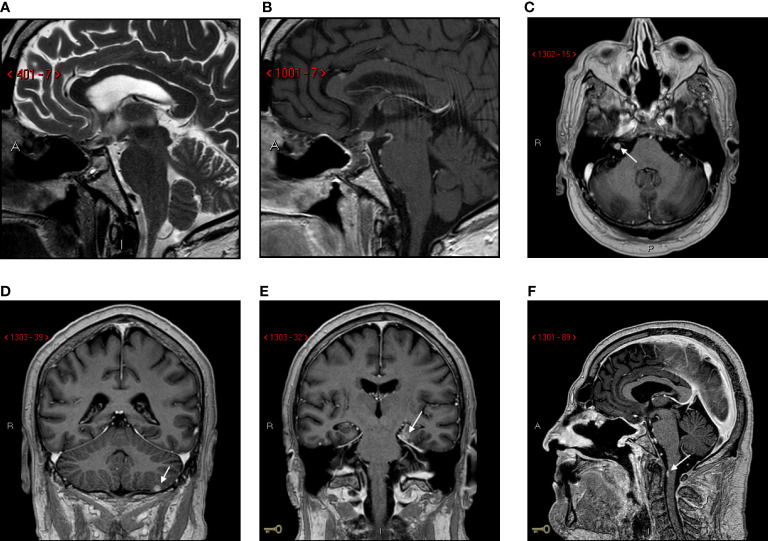
Methods: We present the case of a 58 years-old-man who reported a three-month history of polyuria-polydipsia syndrome, generalized asthenia, panhypopituitarism and bitemporal hemianopsia. Brain-MRI showed a voluminous pituitary mass causing posterior sellar enlargement and compression of the surrounding structures including pituitary stalk, optic chiasm, and optic nerves.
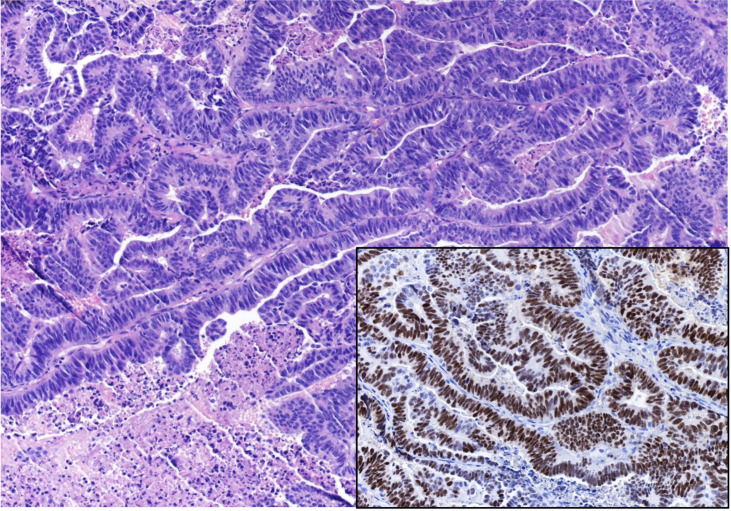
Results: The patient underwent neurosurgical removal of the mass. Histological examination revealed a poorly differentiated adenocarcinoma of uncertain origin. A total body CT scan showed a mass in the left kidney that was subsequently removed. Histological features were consistent with a clear cell carcinoma. However, endoscopic examination of the digestive tract revealed an ulcerating and infiltrating adenocarcinoma of the gastric cardia. Total body PET/CT scan with 18F-FDG confirmed an isolated area of accumulation in the gastric cardia, with no hyperaccumulation at other sites.
Conclusion: To the best of our knowledge, there are no reports of pituitary metastases from gastric cardia adenocarcinoma. Our patient presented with symptoms of sellar involvement and without evidence of other body metastases. Therefore, sudden onset of diabetes insipidus and visual deterioration should lead to the suspicion of a rapidly growing pituitary mass, which may be the presenting manifestation of a primary extracranial adenocarcinoma. Histological investigation of the pituitary mass can guide the diagnostic workup, which must however be complete.
Keywords: diabetes insipidus - neurogenic/central; gastroesophageal junction adenocarcinoma; hypopituitarism; pituitary metastasis; visual disturbance.
Copyright © 2023 Ghezzi, Rossi, Cavallieri, Napoli, Pascarella, Rizzi, Russo, Salomone, Romano, Iaccarino, Froio, Serra, Cozzi, Giaccherini, Valzania and Pisanello.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Diabetes insipidus and panhypopituitarism as a first presentation of silent adenocarcinoma of lung: a case report and literature review.BMC Endocr Disord. 2019 Oct 29;19(1):114. doi: 10.1186/s12902-019-0445-5. BMC Endocr Disord. 2019. PMID: 31664980 Free PMC article. Review.
-
Multiple endocrinological failures as a clinical presentation of a metastatic lung adenocarcinoma.Endocrinol Diabetes Metab Case Rep. 2020 Apr 29;2020:20-0024. doi: 10.1530/EDM-20-0024. Online ahead of print. Endocrinol Diabetes Metab Case Rep. 2020. PMID: 32478672 Free PMC article.
-
Symptomatic Pituitary Metastasis as Initial Manifestation of Renal Cell Carcinoma: Case Report and Review of Literature.Case Rep Endocrinol. 2020 Aug 18;2020:8883864. doi: 10.1155/2020/8883864. eCollection 2020. Case Rep Endocrinol. 2020. PMID: 32908722 Free PMC article.
-
A case of pituitary metastasis from breast cancer that presented as left visual disturbance.J Korean Neurosurg Soc. 2012 Feb;51(2):94-7. doi: 10.3340/jkns.2012.51.2.94. Epub 2012 Feb 29. J Korean Neurosurg Soc. 2012. PMID: 22500201 Free PMC article.
-
[Lymphocytic infundibulo-hypophysitis with diabetes insipidus as a new clinical entity: a case report and review of the literature].No Shinkei Geka. 1997 Feb;25(2):169-75. No Shinkei Geka. 1997. PMID: 9027895 Review. Japanese.
References
Publication types
LinkOut - more resources
Full Text Sources