

Review
doi: 10.1016/j.bjae.2022.11.005.
Epub 2022 Dec 21.
Antiarrhythmic drugs and anaesthesia. Part 2: pharmacotherapy
Affiliations
- PMID: 36686887
- PMCID: PMC9845544
- DOI: 10.1016/j.bjae.2022.11.005
Item in Clipboard
Review
Antiarrhythmic drugs and anaesthesia. Part 2: pharmacotherapy
BJA Educ.
2023 Feb.
No abstract available
Keywords: antiarrhythmic agents; arrhythmias; cardiac; cardiac electrophysiology.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
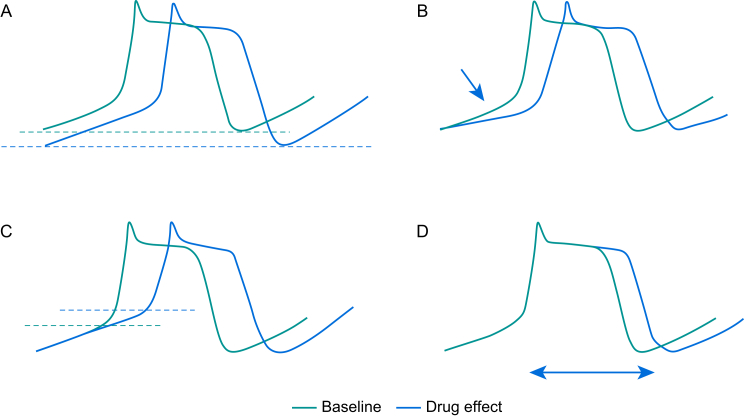
Automaticity can be suppressed by (A) hyperpolarisation of the RMP, (B) reducing the slope of pacemaker potential (phase 4), (C) increasing the threshold potential, (D) increasing the action potential duration.
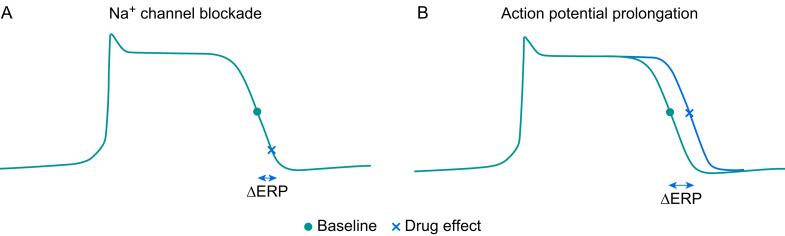
(A) Na+ channel blockers delay the point at which Na+ channels recover from an inactivated state, thereby increasing the effective refractory period (ERP). (B) K+ channel blockers prolong the action potential duration, increasing the ERP.
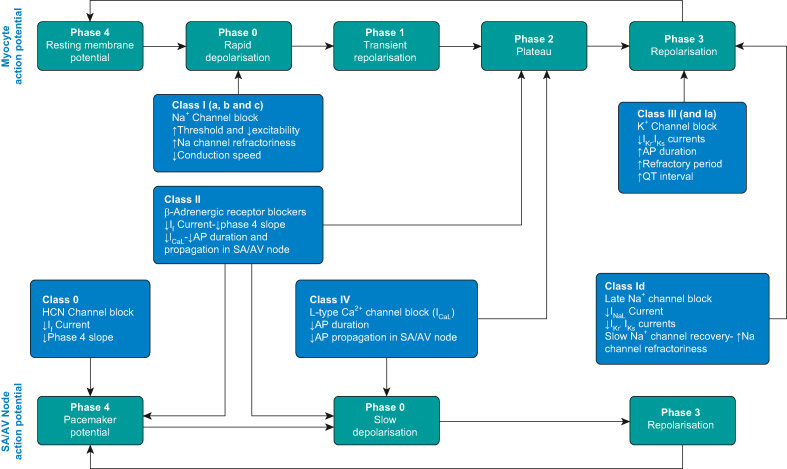
Summary of mechanism of actions of antiarrhythmic drug. AP, action potential.
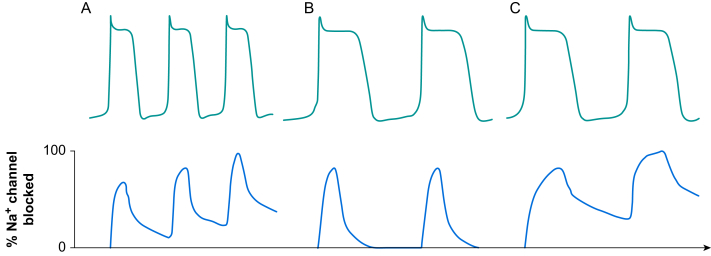
Dissociation kinetics of Na+ channel blockers. Na+ channel blockers bind to Na+ channels in the open or inactivated states. Dissociation kinetics of the blockers and recovery of channels during diastole determines the extent of Na+ channel blockade. (A) Class Ia drugs have an intermediate dissociation rate and Na+ channel blockade is influenced by the heart rate. As the heart rate increases, the time available for drugs to dissociate from the channels during diastole is reduced. This increases level of Na+ channel blockade and provides heart rate-dependent steady state Na+ blockade. (B) Class Ib drugs have rapid dissociation kinetics allowing full recovery of Na+ channels before the next action potential. (C) Class Ic drugs have slow dissociation kinetics. The drugs do not completely dissociate from the Na+ channels even at low heart rate. This results in steady-state Na+ channel blockade even when the cell membrane is fully repolarised.
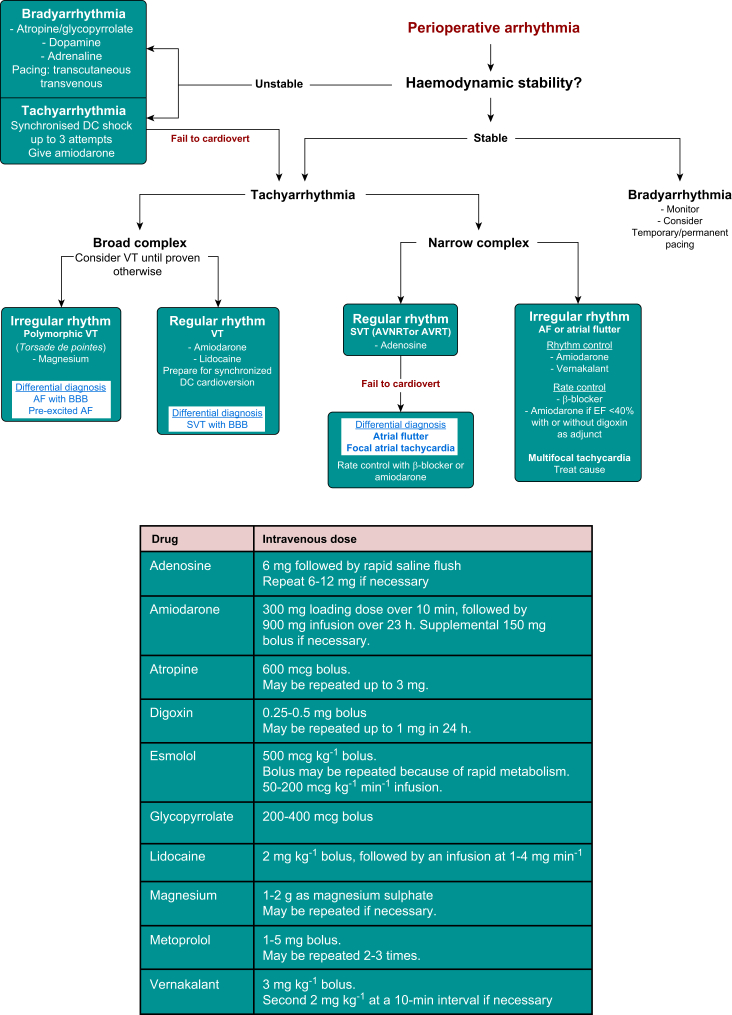
Common perioperative arrhythmias and management algorithm. Doses of commonly used antiarrhythmic drugs. AVNRT, atrioventricular node re-entry tachycardia; AVRT, atrioventricular re-entry tachycardia; BBB, bundle branch block; EF, ejection fraction; SVT, supraventricular tachycardia; VT, ventricular tachycardia.
Similar articles
-
Antiarrhythmic drugs and anaesthesia: part 1. mechanisms of cardiac arrhythmias.BJA Educ. 2023 Jan;23(1):8-16. doi: 10.1016/j.bjae.2022.11.001. Epub 2022 Dec 5. BJA Educ. 2023. PMID: 36601026 Free PMC article. Review. No abstract available.
-
Pharmacotherapy of cardiac arrhythmias--basic science for clinicians.Pacing Clin Electrophysiol. 2009 Nov;32(11):1454-65. doi: 10.1111/j.1540-8159.2009.02526.x. Epub 2009 Sep 10. Pacing Clin Electrophysiol. 2009. PMID: 19744278 Review.
-
Future of antiarrhythmic drugs.Curr Opin Cardiol. 2006 Jul;21(4):361-7. doi: 10.1097/01.hco.0000231407.61683.05. Curr Opin Cardiol. 2006. PMID: 16755206 Review.
-
Model systems for the discovery and development of antiarrhythmic drugs.Prog Biophys Mol Biol. 2008 Oct-Nov;98(2-3):328-39. doi: 10.1016/j.pbiomolbio.2008.10.009. Epub 2008 Nov 11. Prog Biophys Mol Biol. 2008. PMID: 19038282 Review.
-
Predicting the recurrence of ventricular tachyarrhythmias from T-wave alternans assessed on antiarrhythmic pharmacotherapy: a prospective study in patients with dilated cardiomyopathy.Ann Noninvasive Electrocardiol. 2001 Jul;6(3):203-8. doi: 10.1111/j.1542-474x.2001.tb00109.x. Ann Noninvasive Electrocardiol. 2001. PMID: 11466138 Free PMC article.
References
-
- Harvey R.D., Grant A.O. In: Basic & clinical pharmacology. 15th Edn. Katzung B.G., Vanderah T.W., editors. McGraw-Hill; New York: 2021. Agents used in cardiac arrhythmias.
-
- Grant A.O. Cardiac ion channels. Circ Arrhythm Electrophysiol. 2009;2:185–194. - PubMed
-
- Dan G.A., Martinez-Rubio A., Agewall S., et al. Antiarrhythmic drugs – clinical use and clinical decision making: a consensus document from the EHRA and ESC Working Group on Cardiovascular Pharmacology, endorsed by the HRS, APHRS and ISCP. Europace. 2018;20:731–732. - PubMed
-
- Stewart A.M., Greaves K., Bromilow J. Supraventricular tachyarrhythmias and their management in the perioperative period. Cont Educ Anaesth Crit Care Pain. 2015;15:90–97.
Publication types
LinkOut - more resources
Full Text Sources
