

The Role of Impulse Oscillometry in Evaluating Disease Severity and Predicting the Airway Reversibility in Patients With Bronchiectasis
- PMID: 36687424
- PMCID: PMC9847491
- DOI: 10.3389/fmed.2022.796809
The Role of Impulse Oscillometry in Evaluating Disease Severity and Predicting the Airway Reversibility in Patients With Bronchiectasis
Abstract
Background: Impulse oscillometry (IOS) can be used to evaluate airway impedance in patients with obstructive airway diseases. Previous studies have demonstrated that IOS parameters differ between patients with bronchiectasis and healthy controls. This study aims to explore the usefulness of IOS in assessing disease severity and airway reversibility in patients with bronchiectasis.
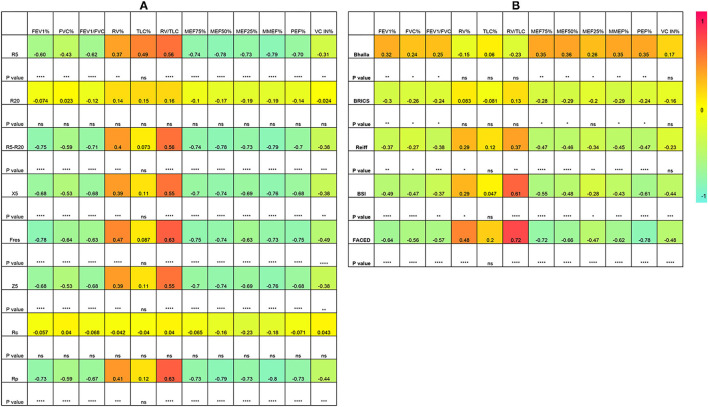
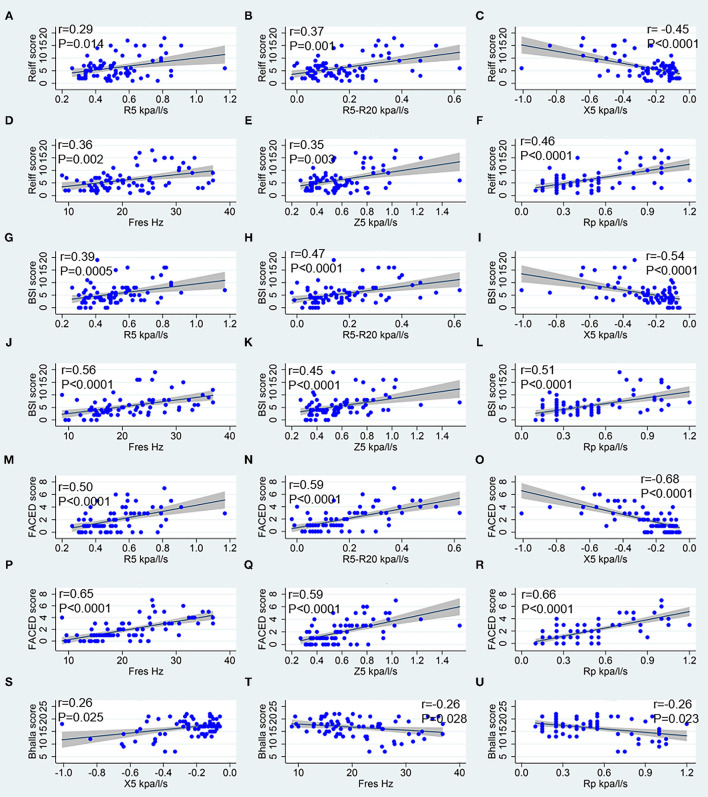
Method: Seventy-four patients with non-cystic fibrosis bronchiectasis who visited our Respiratory Medicine outpatient clinic were consecutively recruited. Spirometry, plethysmography and IOS tests were performed. Patients were stratified into mild, moderate and severe disease according to Reiff, Bhalla, BSI, FACED, and BRICS scores. Airway reversibility was measured by bronchodilation test (BDT) and the result was classified as positive or negative. ROC curves of IOS parameters were used to assess the usefulness of IOS parameters in predicting airway reversibility. Correlations between the IOS, spirometric lung function and bronchiectasis severity parameters were analyzed.
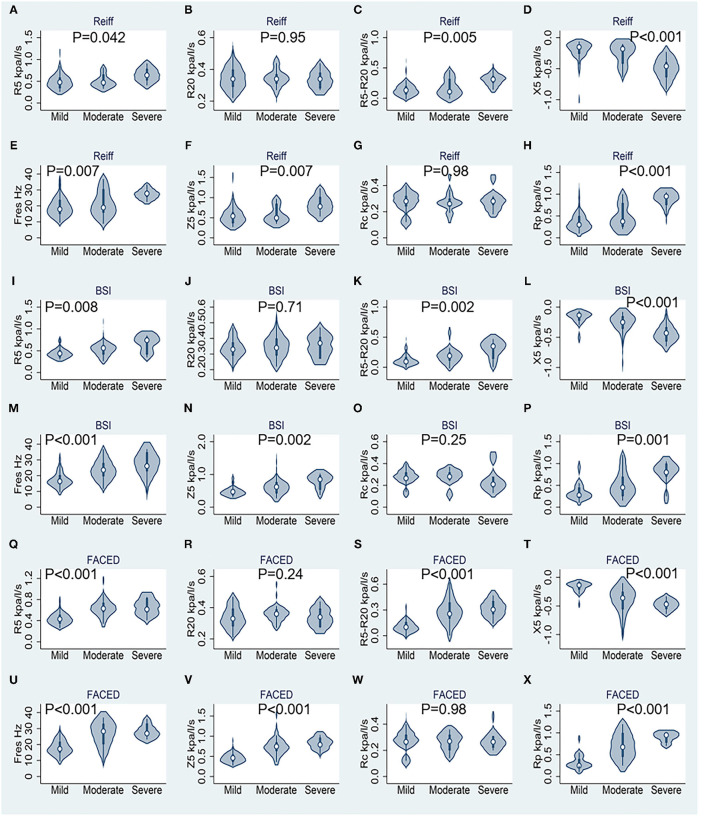
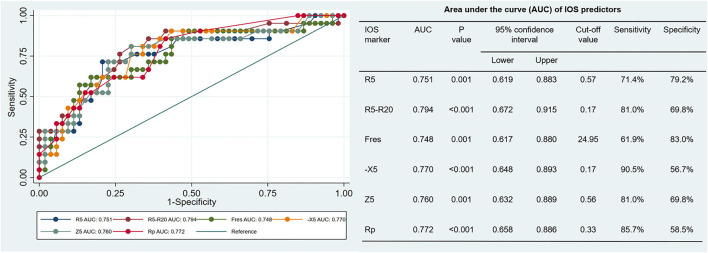
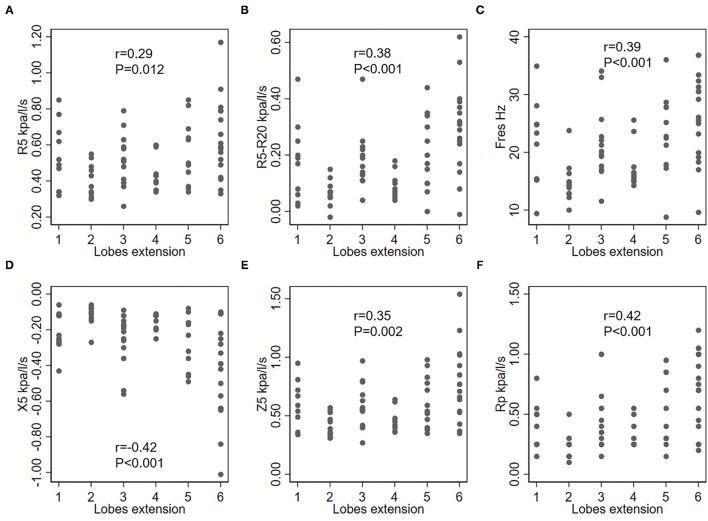
Results: Many IOS parameters, such as airway resistance at 5 Hz (R5), small airways resistance (R5-R20), total airway reactance (X5), resonance frequency (Fres), total airway impedance at 5 Hz (Z5), and peripheral resistance (Rp) increased in patients with bronchiectasis who presented a moderate to severe severity as categorized by the FACED, BSI and Reiff scores. Large airway resistance (R20) and central resistance (Rc) were not significantly different among groups with different bronchiectasis severity. The difference between R5 and R20 (R5-R20) showed 81.0% sensitivity, and 69.8%specificity in predicting the airway reversibility in bronchiectasis with AUC of 0.794 (95%CI, 0.672-0.915).
Conclusion: IOS measurements are useful indicators of bronchiectasis severity and may be useful for predicting the airway reversibility.
Keywords: airway reversibility; bronchiectasis; impulse oscillometry; plethysmography; spirometry.
Copyright © 2022 Tan, Ma, Wang, Tu, Chen, Zheng, Liang, Huang, Wang, Wu, Huang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Usefulness of Impulse Oscillometry in Predicting the Severity of Bronchiectasis.Tuberc Respir Dis (Seoul). 2024 Jul;87(3):368-377. doi: 10.4046/trd.2023.0160. Epub 2024 Apr 30. Tuberc Respir Dis (Seoul). 2024. PMID: 38783483 Free PMC article.
-
Comparative evaluation of expiratory airflow limitation between patients with COPD and BE using IOS.Sci Rep. 2021 Feb 25;11(1):4524. doi: 10.1038/s41598-021-84028-9. Sci Rep. 2021. PMID: 33633234 Free PMC article.
-
[Correlation of Impulse oscillometry system indices with conventional pulmonary function tests in patients with obstructive pulmonary ventilation dysfunction].Zhonghua Nei Ke Za Zhi. 2024 Nov 1;63(11):1087-1095. doi: 10.3760/cma.j.cn112138-20240410-00231. Zhonghua Nei Ke Za Zhi. 2024. PMID: 39482072 Chinese.
-
Clinical Value of Impulse Oscillometry in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis.Respiration. 2025;104(2):100-109. doi: 10.1159/000541633. Epub 2024 Oct 3. Respiration. 2025. PMID: 39362193
-
What can we learn about COPD from impulse oscillometry?Respir Med. 2018 Jun;139:106-109. doi: 10.1016/j.rmed.2018.05.004. Epub 2018 May 16. Respir Med. 2018. PMID: 29857993 Review.
Cited by
-
Impact of Aerobika® oscillating positive expiratory pressure in improving small airway resistance, lung function, symptoms and exercise capacity in chronic obstructive pulmonary disease.Front Med (Lausanne). 2023 Jun 2;10:1202380. doi: 10.3389/fmed.2023.1202380. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37332765 Free PMC article.
-
Usefulness of Impulse Oscillometry in Predicting the Severity of Bronchiectasis.Tuberc Respir Dis (Seoul). 2024 Jul;87(3):368-377. doi: 10.4046/trd.2023.0160. Epub 2024 Apr 30. Tuberc Respir Dis (Seoul). 2024. PMID: 38783483 Free PMC article.
-
Bronchiectasis Assessment in Primary Ciliary Dyskinesia: A Non-Invasive Approach Using Forced Oscillation Technique.Diagnostics (Basel). 2023 Jul 6;13(13):2287. doi: 10.3390/diagnostics13132287. Diagnostics (Basel). 2023. PMID: 37443681 Free PMC article.
-
Quantitative CT Metrics for the Prediction of Therapeutic Effect in Asthma.J Clin Med. 2023 Jan 13;12(2):639. doi: 10.3390/jcm12020639. J Clin Med. 2023. PMID: 36675568 Free PMC article.
References
LinkOut - more resources
Full Text Sources