

Successful hepatic resection for invasive Klebsiella pneumoniae large multiloculated liver abscesses with percutaneous drainage failure: A case report
- PMID: 36687430
- PMCID: PMC9852881
- DOI: 10.3389/fmed.2022.1092879
Successful hepatic resection for invasive Klebsiella pneumoniae large multiloculated liver abscesses with percutaneous drainage failure: A case report
Abstract
Background: Invasive Klebsiella-associated liver abscesses can progress rapidly and cause severe metastatic infections such as meningitis and hydrocephalus, which are associated with high morbidity and mortality. In patients with large multiloculated liver abscesses after failure of percutaneous drainage, rapid diagnosis of the abscess followed by hepatic resection is necessary for early recovery and to prevent severe secondary metastatic complications.
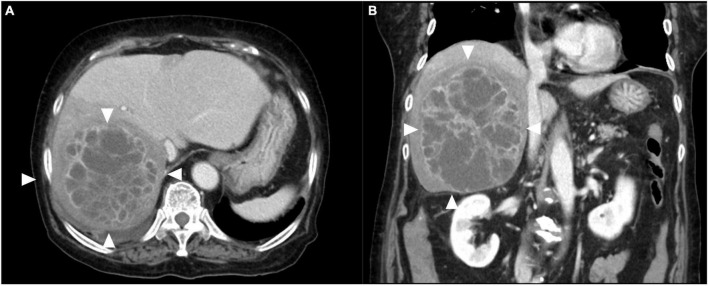
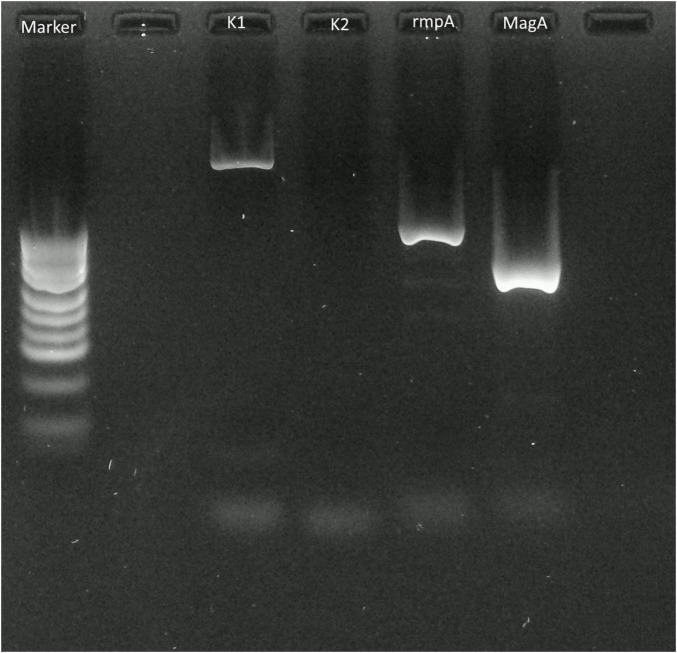
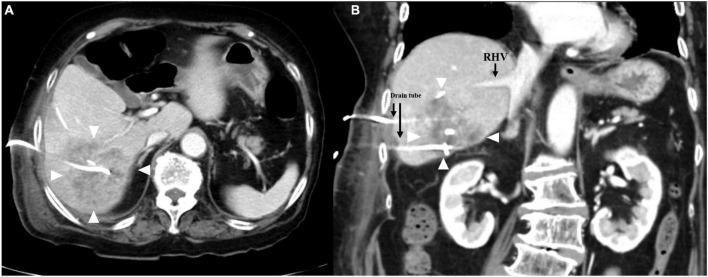
Case presentation: An 84-year-old woman with a large liver abscess and in septic shock was transferred to our hospital. Abdominal CT showed multiloculated liver abscesses 15 cm in diameter in the right lobe of the liver. We first performed percutaneous liver abscess drainage. The patient was managed in the intensive care unit, as well as treated with intravenous administration of meropenem followed by cefozopran according to the antibiogram. Klebsiella pneumoniae with invasive infection was confirmed by a string test in an isolated colony of K. pneumoniae; the K1 serotype with the rmpA and magA genes was determined by polymerase chain reaction and Sanger sequencing. Additional percutaneous liver abscess drainage was performed due to initial inadequate drainage. Although the abscess had shrunk to a diameter of 8 cm after drainage in 4 weeks, the patient recovered from sepsis, but still had low-grade fever (occasionally 38°C) and continued to have symptoms of chronic inflammation with persistent hyper mucus discharge from the liver abscess. Surgical resection was chosen to prevent prolonged hospitalization and ensure early recovery. A right posterior sectionectomy of the liver, including liver abscess, was performed. The post-operative course was uneventful, with no complications, and she was discharged after 18 days. There were no signs of abscess recurrence 1 year after surgery.
Conclusion: We present a case of successful hepatic resection after percutaneous drainage failure in a patient with invasive K. pneumoniae multiloculated liver abscess.
Keywords: K. pneumoniae; K1 serotype; Klebsiella-associated multiloculated liver abscess; hyper mucus discharge; percutaneous drainage failure.
Copyright © 2023 Nojima, Shimizu, Murakami, Yamazaki, Yamazaki, Suzuki, Shuto, Kosugi, Usui and Koda.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Two unusual cases of successful treatment of hypermucoviscous Klebsiella pneumoniae invasive syndrome.BMC Infect Dis. 2016 Nov 16;16(1):680. doi: 10.1186/s12879-016-2011-3. BMC Infect Dis. 2016. PMID: 27852233 Free PMC article.
-
Invasive liver abscess syndrome caused by Klebsiella pneumoniae with definite K2 serotyping in Japan: a case report.Surg Case Rep. 2016 Dec;2(1):72. doi: 10.1186/s40792-016-0201-2. Epub 2016 Jul 25. Surg Case Rep. 2016. PMID: 27457077 Free PMC article.
-
Predictors of septic metastatic infection and mortality among patients with Klebsiella pneumoniae liver abscess.Clin Infect Dis. 2008 Sep 1;47(5):642-50. doi: 10.1086/590932. Clin Infect Dis. 2008. PMID: 18643760
-
Percutaneous management of pyogenic hepatic abscesses.HPB Surg. 1990 Jul;2(3):185-8. doi: 10.1155/1990/28345. HPB Surg. 1990. PMID: 2278915 Free PMC article. Review.
-
Klebsiella pneumoniae-induced multiple invasive abscesses: A case report and literature review.Medicine (Baltimore). 2019 Sep;98(39):e17362. doi: 10.1097/MD.0000000000017362. Medicine (Baltimore). 2019. PMID: 31574882 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources