

Evaluation of adalimumab effects on left ventricle performance by echocardiography indexes among patients with immunosuppressant refractory ulcerative colitis
- PMID: 36687438
- PMCID: PMC9853977
- DOI: 10.3389/fmed.2022.1008711
Evaluation of adalimumab effects on left ventricle performance by echocardiography indexes among patients with immunosuppressant refractory ulcerative colitis
Abstract
Background and aims: Inflammatory bases lead to a simultaneous flourishing of cardiovascular complications with inflammatory bowel disease (IBD). As a released cytokine, tumor necrosis factor-α (TNF-α) can either disrupt or preserve cardiovascular performance. Due to this controversy, this study aimed to appraise the short-term anti-TNF (adalimumab [ADA]) relics on cardiac function by gauging the echocardiography indexes in patients with immunosuppressant refractory ulcerative colitis (UC).
Methods: All cases with a definite diagnosis of UC were included based on providing written informed consent and owning the severe form of active disease (Mayo score ≥7), which did not dampen with immunosuppressant. Patients were excluded in the case of previous cardiac ailments/risk factors and prior related surgical or pharmaceutical intervention. Transthoracic echocardiography (TTE) was carried out before and 3 months after biological regimen allocation and changes in indexes [ejection fraction (EF), left ventricular end-diastolic volume (LVEDV)/left ventricular end-systolic volume (LVESV), and global longitudinal strain (GLS) in standard parasternal short axis from mid-ventricular level, two-, three-, and four-chamber apical long axes] were compared via statistical analyses.
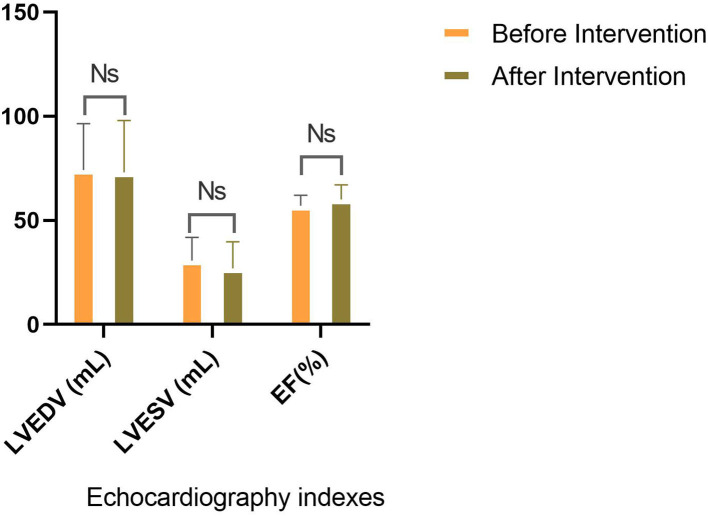
Results: The study consisted of 13 (65%) men and 7 (35%) women, with a mean age of 36.54 ± 11.3 years. Participants mainly possessed Montreal class I (45%) and an average of 3.25 years of disease duration. The intervention significantly controlled inflammation [endoscopic Mayo score (P = 0.001), partial Mayo score (P = 0.001), and C-reactive protein (P = 0.001)]. Endoscopic and clinical remission was obtained in 7 (35%) and 9 (45%) patients, respectively; however, no significant discrepancy related to the LVEDV (P = 0.86), LVESV (P-value = 0.25), EF (P-value = 0.06), and GLS in standard parasternal short axis (P = 0.73), long axis [apical 2-chamber (P-value = 0.61), apical 3-chamber (P-value = 0.15), and apical 4-chamber (P-value = 0.19) views] was observed before and after the intervention. Furthermore, no statistically significant correlation between disease activity and cardiac function was found, neither before nor after ADA administration.
Conclusion: The present perusal found no deterioration in left ventricular function indexes with ADA intervention among patients with IBD without cardiac ailment. Thus, prescribing the anti-TNF to alleviate the inflammation can be carried out with less concern about cardiac consequences and considering other adverse traces in the target group.
Keywords: adalimumab; anti-TNF-α; echocardiography; heart failure; inflammatory bowel disease; longitudinal global strain; ulcerative colitis; vascular stiffness.
Copyright © 2023 Hatamnejad, Karvandi, Jodatfar, Ebrahimi, Shojaeian, Baradaran Ghavami, Balaii, Moeeni, Rajabnia, Shahrokh and Asadzadeh Aghdaei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
The apical long-axis rather than the two-chamber view should be used in combination with the four-chamber view for accurate assessment of left ventricular volumes and function.Eur Heart J. 1997 Jul;18(7):1175-85. doi: 10.1093/oxfordjournals.eurheartj.a015414. Eur Heart J. 1997. PMID: 9243153
-
CT-derived left ventricular global strain: a head-to-head comparison with speckle tracking echocardiography.Int J Cardiovasc Imaging. 2019 Sep;35(9):1701-1707. doi: 10.1007/s10554-019-01596-8. Epub 2019 Apr 5. Int J Cardiovasc Imaging. 2019. PMID: 30953252
-
Diagnosis and Management of Cirrhotic Cardiomyopathy.J Clin Exp Hepatol. 2022 Jan-Feb;12(1):186-199. doi: 10.1016/j.jceh.2021.08.016. Epub 2021 Aug 21. J Clin Exp Hepatol. 2022. PMID: 35068798 Free PMC article.
-
European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation.Eur Heart J Cardiovasc Imaging. 2015 Sep;16(9):919-48. doi: 10.1093/ehjci/jev139. Epub 2015 Jul 2. Eur Heart J Cardiovasc Imaging. 2015. PMID: 26139361 Review.
-
TNF inhibitors to treat ulcerative colitis in a metastatic breast cancer patient: a case report and literature review.World J Gastroenterol. 2014 May 21;20(19):5912-7. doi: 10.3748/wjg.v20.i19.5912. World J Gastroenterol. 2014. PMID: 24914353 Free PMC article. Review.
Cited by
-
The anti-inflammatory effects of antidepressants on colitis.Gastroenterol Hepatol Bed Bench. 2024;17(1):28-36. doi: 10.22037/ghfbb.v17i1.2850. Gastroenterol Hepatol Bed Bench. 2024. PMID: 38737937 Free PMC article.
-
Translation and cross-cultural adaptation of the Persian version of inflammatory bowel disease-fatigue (IBD-F) self-assessment questionnaire.PLoS One. 2023 Jul 21;18(7):e0288592. doi: 10.1371/journal.pone.0288592. eCollection 2023. PLoS One. 2023. PMID: 37478140 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous