

Methods on LDL particle isolation, characterization, and component fractionation for the development of novel specific oxidized LDL status markers for atherosclerotic disease risk assessment
- PMID: 36687450
- PMCID: PMC9851470
- DOI: 10.3389/fmed.2022.1078492
Methods on LDL particle isolation, characterization, and component fractionation for the development of novel specific oxidized LDL status markers for atherosclerotic disease risk assessment
Abstract
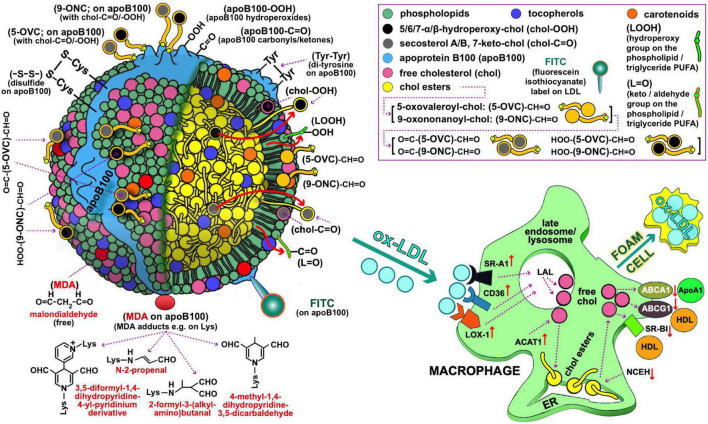
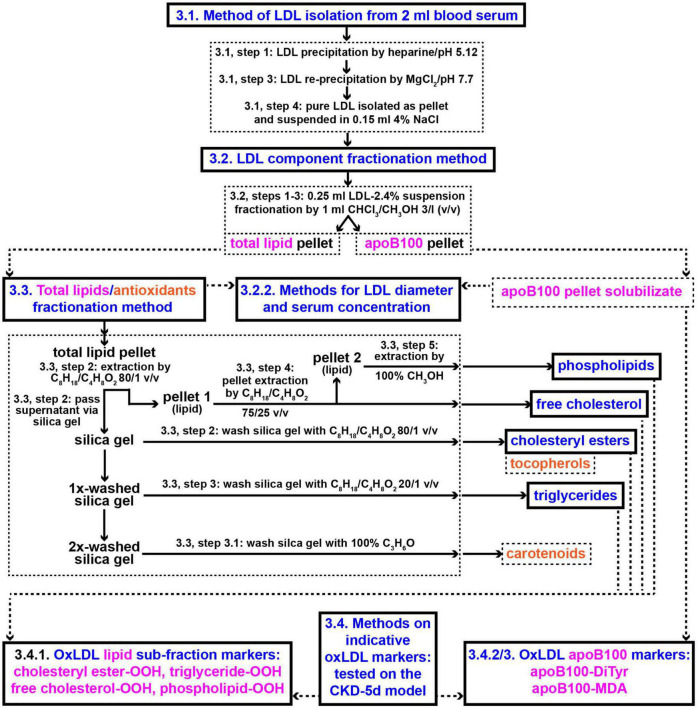
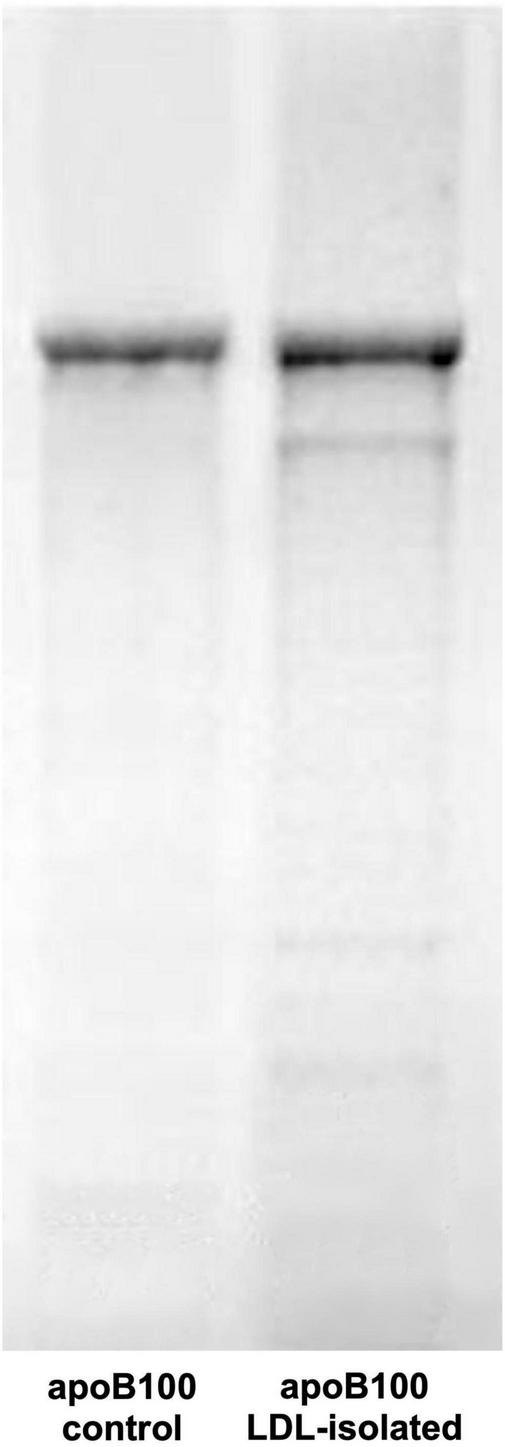
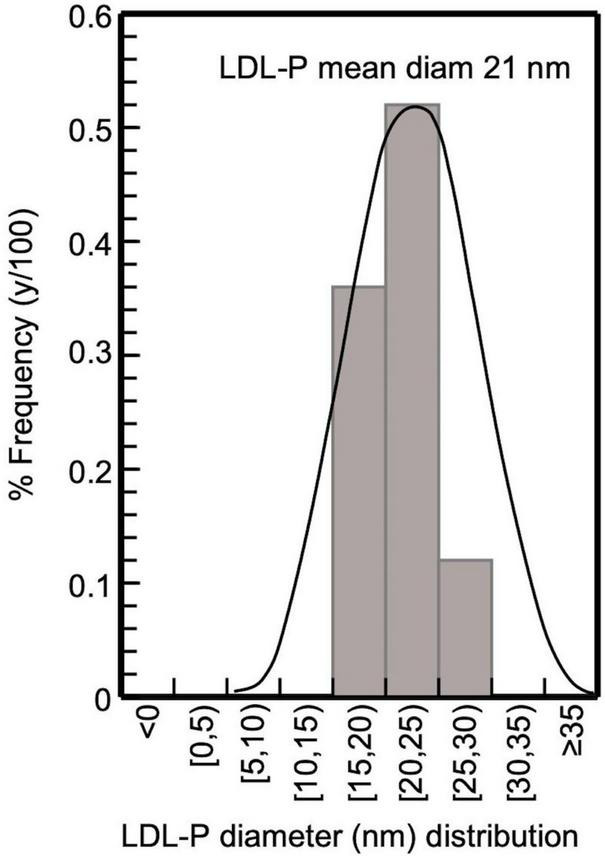
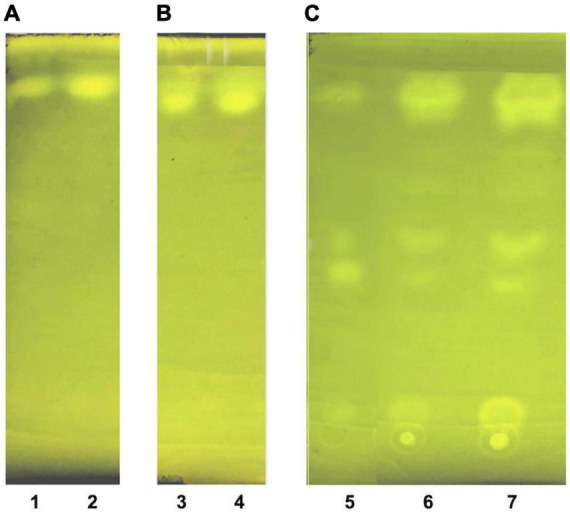
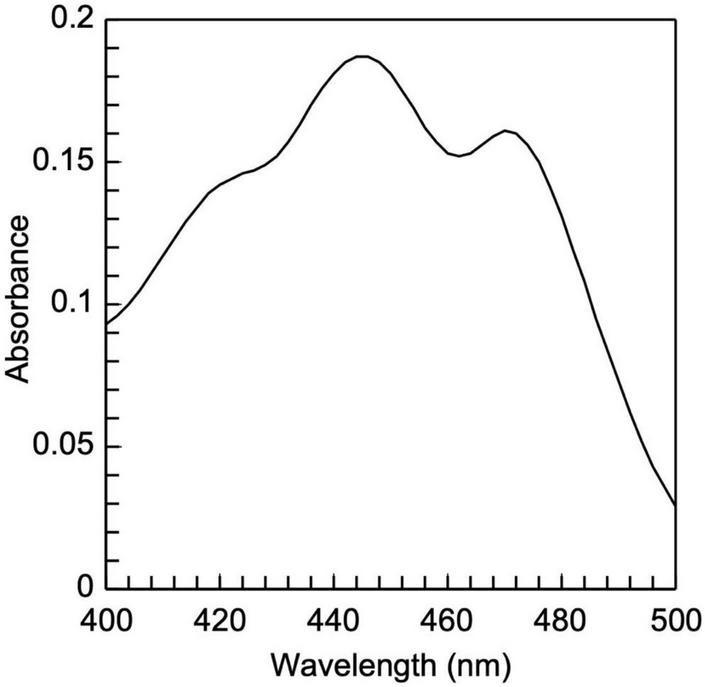
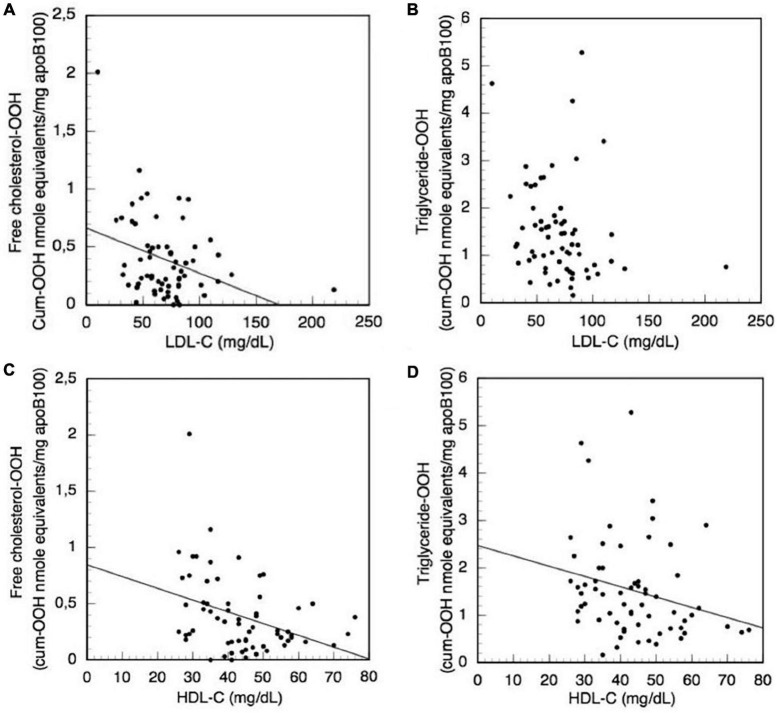
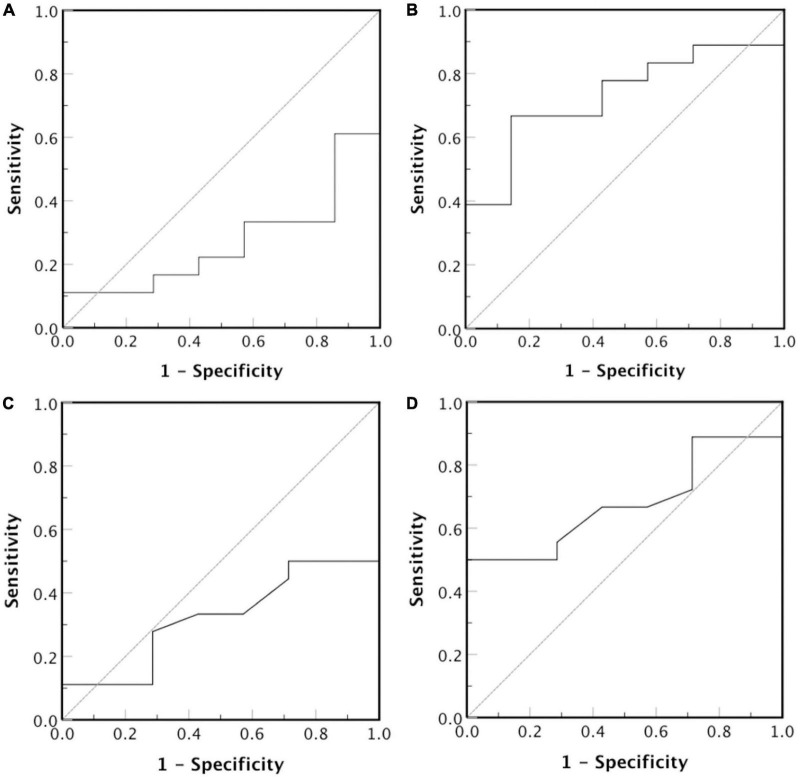
The present study uses simple, innovative methods to isolate, characterize and fractionate LDL in its main components for the study of specific oxidations on them that characterize oxidized low-density lipoprotein (oxLDL) status, as it causatively relates to atherosclerosis-associated cardiovascular disease (CVD) risk assessment. These methods are: (a) A simple, relatively time-short, low cost protocol for LDL isolation, to avoid shortcomings of the currently employed ultracentrifugation and affinity chromatography methodologies. (b) LDL purity verification by apoB100 SDS-PAGE analysis and by LDL particle size determination; the latter and its serum concentration are determined in the present study by a simple method more clinically feasible as marker of CVD risk assessment than nuclear magnetic resonance. (c) A protocol for LDL fractionation, for the first time, into its main protein/lipid components (apoB100, phospholipids, triglycerides, free cholesterol, and cholesteryl esters), as well as into LDL carotenoid/tocopherol content. (d) Protocols for the measurement, for the first time, of indicative specific LDL component oxidative modifications (cholesteryl ester-OOH, triglyceride-OOH, free cholesterol-OOH, phospholipid-OOH, apoB100-MDA, and apoB100-DiTyr) out of the many (known/unknown/under development) that collectively define oxLDL status, which contrasts with the current non-specific oxLDL status evaluation methods. The indicative oxLDL status markers, selected in the present study on the basis of expressing early oxidative stress-induced oxidative effects on LDL, are studied for the first time on patients with end stage kidney disease on maintenance hemodialysis, selected as an indicative model for atherosclerosis associated diseases. Isolating LDL and fractionating its protein and main lipid components, as well as its antioxidant arsenal comprised of carotenoids and tocopherols, paves the way for future studies to investigate all possible oxidative modifications responsible for turning LDL to oxLDL in association to their possible escaping from LDL's internal antioxidant defense. This can lead to studies to identify those oxidative modifications of oxLDL (after their artificial generation on LDL), which are recognized by macrophages and convert them to foam cells, known to be responsible for the formation of atherosclerotic plaques that lead to the various CVDs.
Keywords: HDL-C; LDL lipid fractions; LDL-C; apoB100; atherosclerosis; cardiovascular diseases; clinical markers; oxidized LDL.
Copyright © 2023 Papadea, Skipitari, Kalaitzopoulou, Varemmenou, Spiliopoulou, Papasotiriou, Papachristou, Goumenos, Onoufriou, Rosmaraki, Margiolaki and Georgiou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Novel oxidized LDL-based clinical markers in peritoneal dialysis patients for atherosclerosis risk assessment.Redox Biol. 2023 Aug;64:102762. doi: 10.1016/j.redox.2023.102762. Epub 2023 Jun 2. Redox Biol. 2023. PMID: 37302344 Free PMC article.
-
Serum cholesterol loading capacity of macrophages is regulated by seropositivity and C-reactive protein in rheumatoid arthritis patients.Rheumatology (Oxford). 2023 Mar 1;62(3):1254-1263. doi: 10.1093/rheumatology/keac394. Rheumatology (Oxford). 2023. PMID: 35809057
-
Circulating oxidized LDL: determinants and association with brachial flow-mediated dilation.J Lipid Res. 2009 Feb;50(2):342-9. doi: 10.1194/jlr.P800030-JLR200. Epub 2008 Sep 18. J Lipid Res. 2009. PMID: 18802196
-
Mechanisms of Oxidized LDL-Mediated Endothelial Dysfunction and Its Consequences for the Development of Atherosclerosis.Front Cardiovasc Med. 2022 Jun 1;9:925923. doi: 10.3389/fcvm.2022.925923. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35722128 Free PMC article. Review.
-
[Does Lp-PLA2 determination help predict atherosclerosis and cardiocerebrovascular disease?].Acta Med Croatica. 2010 Oct;64(4):237-45. Acta Med Croatica. 2010. PMID: 21688606 Review. Croatian.
Cited by
-
Efficacy of antioxidant intervention and exercise intervention for lipid peroxidation in dialysis patients: a meta-analysis.Front Med (Lausanne). 2025 Mar 17;12:1473818. doi: 10.3389/fmed.2025.1473818. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40166056 Free PMC article.
-
Novel oxidized LDL-based clinical markers in peritoneal dialysis patients for atherosclerosis risk assessment.Redox Biol. 2023 Aug;64:102762. doi: 10.1016/j.redox.2023.102762. Epub 2023 Jun 2. Redox Biol. 2023. PMID: 37302344 Free PMC article.
-
The Effect of Berry Consumption on Oxidative Stress Biomarkers: A Systematic Review of Randomized Controlled Trials in Humans.Antioxidants (Basel). 2023 Jul 18;12(7):1443. doi: 10.3390/antiox12071443. Antioxidants (Basel). 2023. PMID: 37507981 Free PMC article. Review.
-
We Must Abandon the Myth: Oxidized Low-density Lipoprotein is not a Lipoprotein that Plays a Key Role in Atherogenesis.Curr Med Chem. 2025;32(15):2899-2914. doi: 10.2174/0109298673301236240311113807. Curr Med Chem. 2025. PMID: 38494931 Free PMC article. Review.
References
-
- Pahwa R, Jialal I. Atherosclerosis. Treasure Island, FL: StatPearls Publishing; (2021). - PubMed
-
- Nakanishi R, Baskaran L, Gransar H, Budoff M, Achenbach S, Al-Mallah M, et al. Relationship of hypertension to coronary atherosclerosis and cardiac events in ratients with coronary computed tomographic angiography. Hypertension. (2017) 70:293–9. 10.1161/HYPERTENSIONAHA.117.09402 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources