

Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension
- PMID: 36688507
- PMCID: PMC10685906
- DOI: 10.1056/NEJMoa2212663
Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension
Abstract
Background: Intravenous fluids and vasopressor agents are commonly used in early resuscitation of patients with sepsis, but comparative data for prioritizing their delivery are limited.
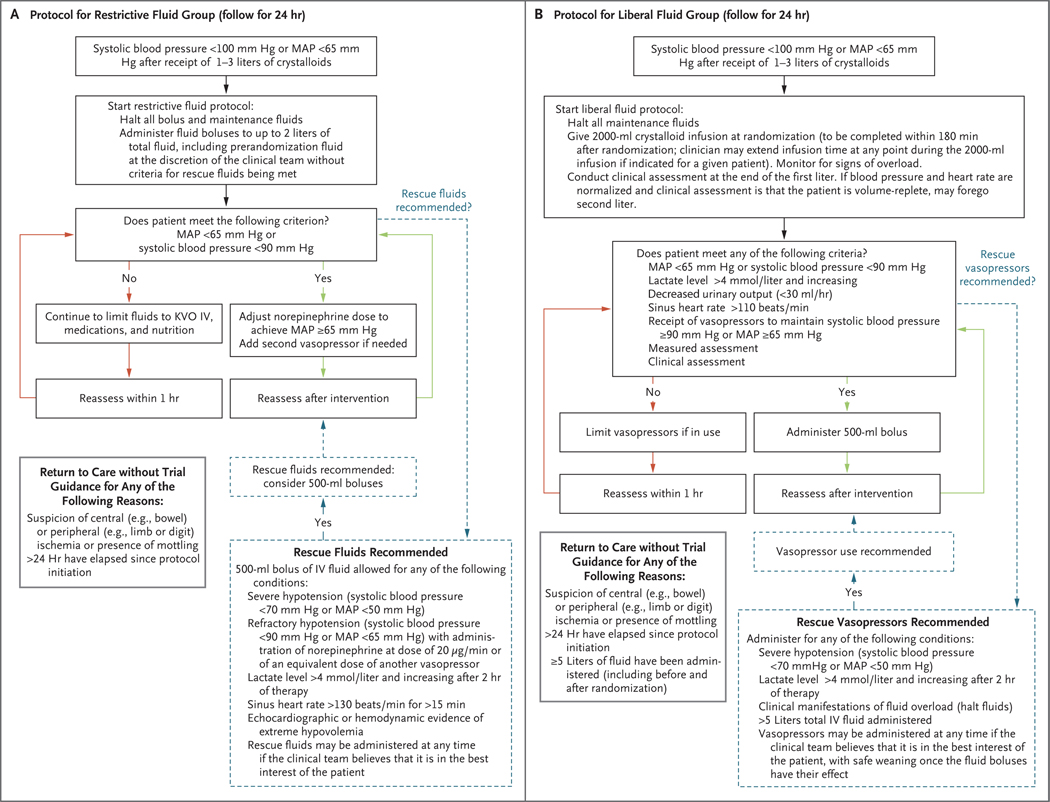
Methods: In an unblinded superiority trial conducted at 60 U.S. centers, we randomly assigned patients to either a restrictive fluid strategy (prioritizing vasopressors and lower intravenous fluid volumes) or a liberal fluid strategy (prioritizing higher volumes of intravenous fluids before vasopressor use) for a 24-hour period. Randomization occurred within 4 hours after a patient met the criteria for sepsis-induced hypotension refractory to initial treatment with 1 to 3 liters of intravenous fluid. We hypothesized that all-cause mortality before discharge home by day 90 (primary outcome) would be lower with a restrictive fluid strategy than with a liberal fluid strategy. Safety was also assessed.
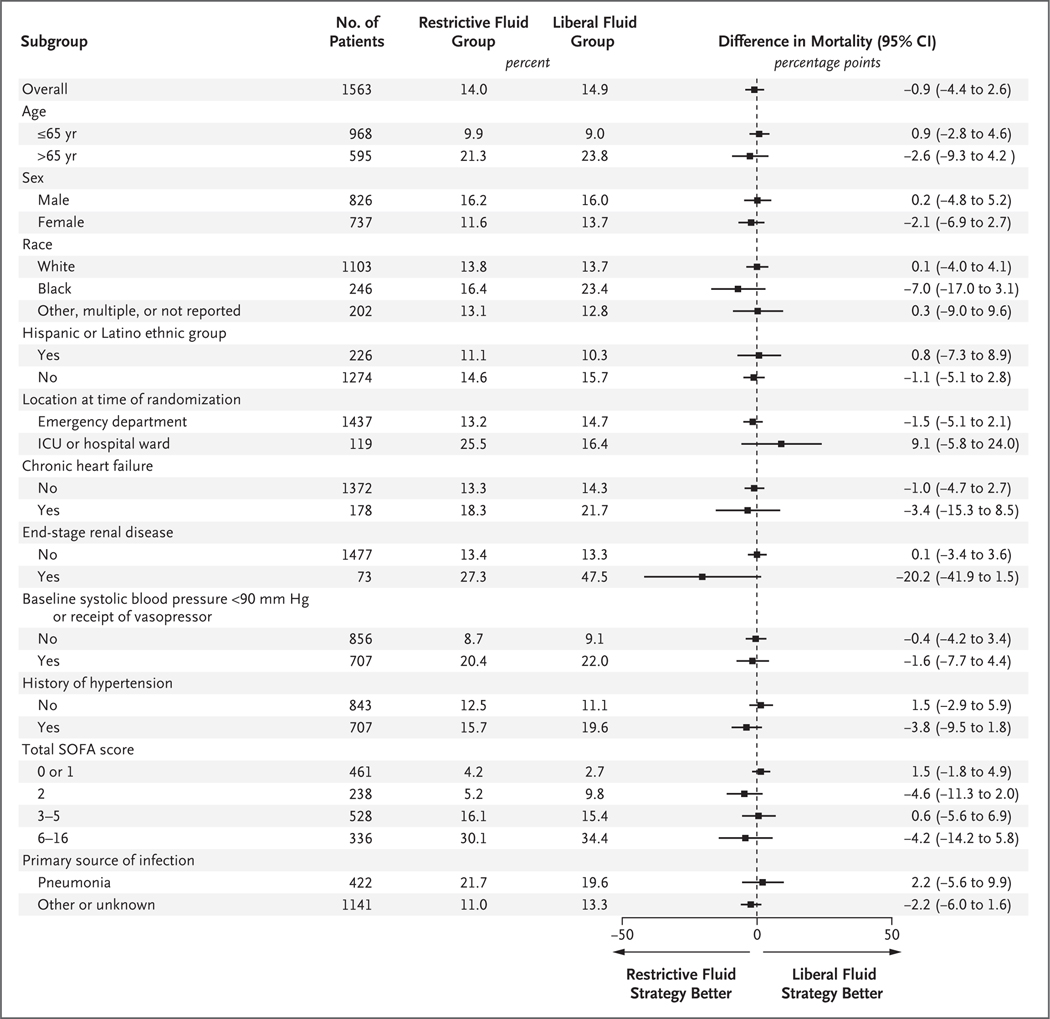
Results: A total of 1563 patients were enrolled, with 782 assigned to the restrictive fluid group and 781 to the liberal fluid group. Resuscitation therapies that were administered during the 24-hour protocol period differed between the two groups; less intravenous fluid was administered in the restrictive fluid group than in the liberal fluid group (difference of medians, -2134 ml; 95% confidence interval [CI], -2318 to -1949), whereas the restrictive fluid group had earlier, more prevalent, and longer duration of vasopressor use. Death from any cause before discharge home by day 90 occurred in 109 patients (14.0%) in the restrictive fluid group and in 116 patients (14.9%) in the liberal fluid group (estimated difference, -0.9 percentage points; 95% CI, -4.4 to 2.6; P = 0.61); 5 patients in the restrictive fluid group and 4 patients in the liberal fluid group had their data censored (lost to follow-up). The number of reported serious adverse events was similar in the two groups.
Conclusions: Among patients with sepsis-induced hypotension, the restrictive fluid strategy that was used in this trial did not result in significantly lower (or higher) mortality before discharge home by day 90 than the liberal fluid strategy. (Funded by the National Heart, Lung, and Blood Institute; CLOVERS ClinicalTrials.gov number, NCT03434028.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Usual Care, Unusual Care, and the Lessons From CLOVERS: April 2023 Annals of Emergency Medicine Journal Club.Ann Emerg Med. 2023 Apr;81(4):513-515. doi: 10.1016/j.annemergmed.2023.02.005. Ann Emerg Med. 2023. PMID: 36948690 No abstract available.
References
-
- Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med 2021; 49(11):e 1063–e1143. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:1 368–77. - PubMed
-
- Angus DC, Barnato AE, Bell D, et al. A systematic review and meta-analysis of early goal-directed therapy for septic shock: the ARISE, ProCESS and ProMISe Investigators. Intensive Care Med 2015; 41: 1549–60. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL123018/HL/NHLBI NIH HHS/United States
- U01 HL123031/HL/NHLBI NIH HHS/United States
- U01 HL123020/HL/NHLBI NIH HHS/United States
- U01 HL122989/HL/NHLBI NIH HHS/United States
- U01 HL123004/HL/NHLBI NIH HHS/United States
- U01 HL123008/HL/NHLBI NIH HHS/United States
- U01 HL123022/HL/NHLBI NIH HHS/United States
- U01 HL123023/HL/NHLBI NIH HHS/United States
- U01 HL123027/HL/NHLBI NIH HHS/United States
- U01 HL122998/HL/NHLBI NIH HHS/United States
- U01 HL123009/HL/NHLBI NIH HHS/United States
- U01 HL122989, U01 HL122998, U01 HL123004, U01 HL12/HL/NHLBI NIH HHS/United States
- U01 HL123033/HL/NHLBI NIH HHS/United States
- U01 HL123010/HL/NHLBI NIH HHS/United States