

Long-term follow-up of an IgA nephropathy cohort: outcomes and risk factors
- PMID: 36688795
- PMCID: PMC9873278
- DOI: 10.1080/0886022X.2022.2152694
Long-term follow-up of an IgA nephropathy cohort: outcomes and risk factors
Abstract
Aim: IgA nephropathy (IgAN), the most common glomerulopathy worldwide and in Uruguay, raised treatment controversies. The study aimed to analyze long-term IgAN outcomes and treatment.
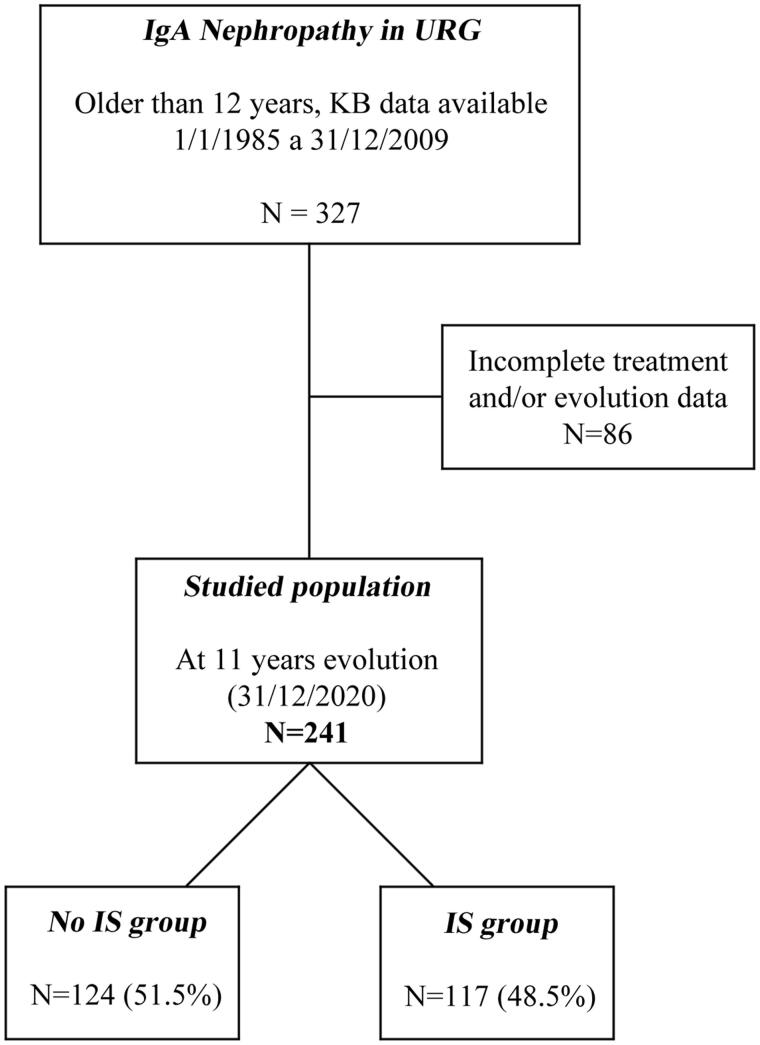
Methods: A retrospective analysis of a Uruguayan IgAN cohort, enrolled between 1985 and 2009 and followed up until 2020, was performed. The Ethics Committee approved the study. The inclusion criteria were (a) biopsy-proven IgAN; (b) age ≥12 years; and (c) available clinical, histologic, and treatment data. The patients were divided into two groups, with immunosuppressive (IS) or without (NoIS) treatment. Outcomes (end-stage kidney disease/kidney replacement therapy [ESKD/KRT] or all-cause death) were obtained from mandatory national registries.
Results: The study population included 241 patients (64.7% men), median age 32 (19.5) years, baseline blood pressure <130/80 mmHg in 37%, and microhematuria in 67.5% of patients. Baseline proteinuria, glomerulosclerosis, and a higher crescent percentage were significantly more frequent in the IS group. Proteinuria improved in both groups. Renal survival at 20 years was 74.6% without difference between groups. In the overall population and in the NoIS group, bivariate Cox regression analysis showed that baseline proteinuria, endocapillary hypercellularity, tubule interstitial damage, and crescents were associated with a higher risk of ESKD/KRT or death, but in the IS group, proteinuria and endocapillary hypercellularity were not. In the multivariate Cox analysis, proteinuria in the NoIS group, crescents in the IS group and tubule interstitial damage in both groups were independent risk factors.
Conclusion: The IS group had more severe risk factors than the NoIS group but attained a similar outcome.
Keywords: IgA nephropathy; kidney replacement therapy; outcomes; risk factors.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures



References
-
- Schena F, Nistor I.. Epidemiology of IgA nephropathy: a global perspective. Semin Nephrol. 2018;38(5):435–442. - PubMed
-
- Mazzuchi N, Acosta N, Caorsi H, et al. Programa de prevención y tratamiento de las glomerulopatías. Frecuencia de diagnóstico y de presentación clínica de glomerulopatías en Uruguay. Nefrologia. 2005;25:113–120. - PubMed
-
- Pattrapornpisut P, Avila-Casado C, Reich HN.. IgA nephropathy: core curriculum 2021. Am J Kidney Dis. 2021;78(3):429–441. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous