

CSF rhinorrhoea after endonasal intervention to the skull base (CRANIAL): A multicentre prospective observational study
- PMID: 36688936
- PMCID: PMC9846732
- DOI: 10.3389/fonc.2022.1049627
CSF rhinorrhoea after endonasal intervention to the skull base (CRANIAL): A multicentre prospective observational study
Abstract
Objective: Despite progress in endonasal skull-base neurosurgery, cerebrospinal fluid (CSF) rhinorrhoea remains common and significant. The CRANIAL study sought to determine 1) the scope of skull-base repair methods used, and 2) corresponding rates of postoperative CSF rhinorrhoea in the endonasal transsphenoidal approach (TSA) and the expanded endonasal approach (EEA) for skull-base tumors.
Methods: A prospective observational cohort study of 30 centres performing endonasal skull-base neurosurgery in the UK and Ireland (representing 91% of adult units). Patients were identified for 6 months and followed up for 6 months. Data collection and analysis was guided by our published protocol and pilot studies. Descriptive statistics, univariate and multivariable logistic regression models were used for analysis.
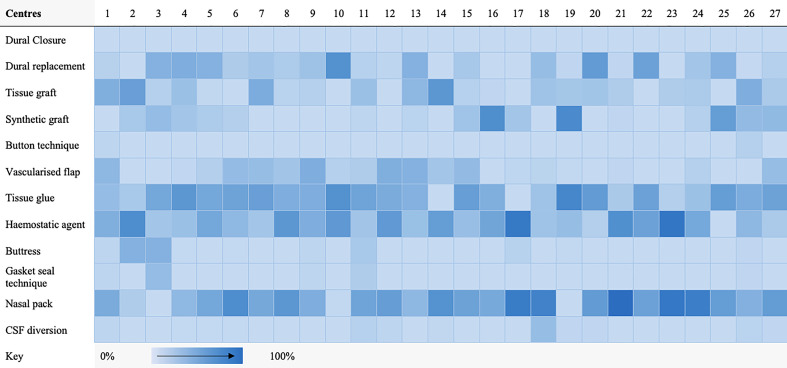
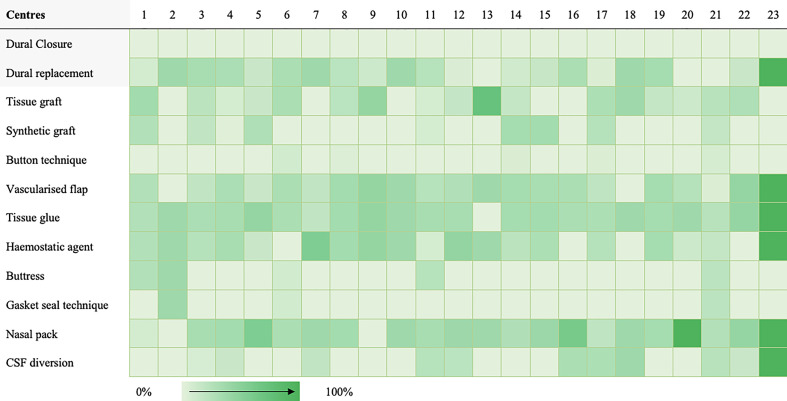
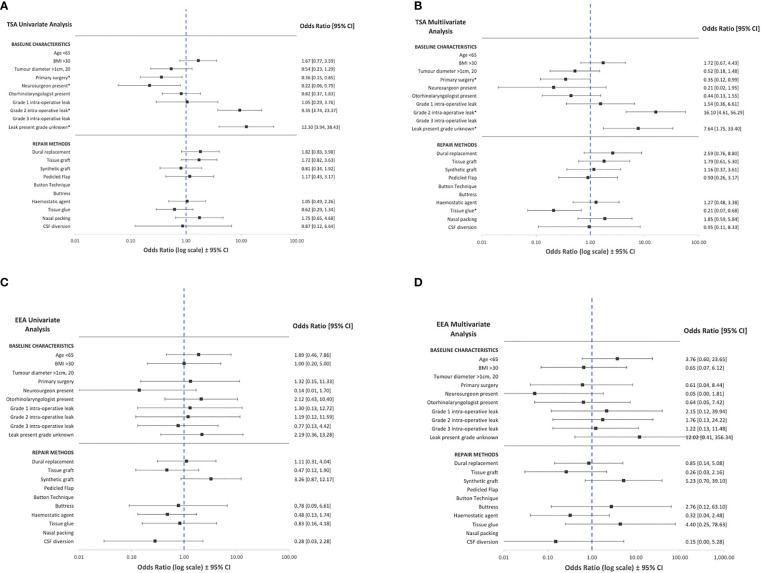
Results: A total of 866 patients were included - 726 TSA (84%) and 140 EEA (16%). There was significant heterogeneity in repair protocols across centres. In TSA cases, nasal packing (519/726, 72%), tissue glues (474/726, 65%) and hemostatic agents (439/726, 61%) were the most common skull base repair techniques. Comparatively, pedicled flaps (90/140, 64%), CSF diversion (38/140, 27%), buttresses (17/140, 12%) and gasket sealing (11/140, 9%) were more commonly used in EEA cases. CSF rhinorrhoea (biochemically confirmed or requiring re-operation) occurred in 3.9% of TSA (28/726) and 7.1% of EEA (10/140) cases. A significant number of patients with CSF rhinorrhoea (15/38, 39%) occurred when no intraoperative CSF leak was reported. On multivariate analysis, there may be marginal benefits with using tissue glues in TSA (OR: 0.2, CI: 0.1-0.7, p<0.01), but no other technique reached significance. There was evidence that certain characteristics make CSF rhinorrhoea more likely - such as previous endonasal surgery and the presence of intraoperative CSF leak.
Conclusions: There is a wide range of skull base repair techniques used across centres. Overall, CSF rhinorrhoea rates across the UK and Ireland are lower than generally reported in the literature. A large proportion of postoperative leaks occurred in the context of occult intraoperative CSF leaks, and decisions for universal sellar repairs should consider the risks and cost-effectiveness of repair strategies. Future work could include longer-term, higher-volume studies, such as a registry; and high-quality interventional studies.
Keywords: CSF; EEA; cerebrospinal fluid leak; cerebrospinal fluid rhinorrhoea; endoscopic endonasal; skull base surgery.
Copyright © 2023 CRANIAL Consortium.
Conflict of interest statement
HM is supported by the Wellcome (203145Z/16/Z) EPSRC (NS/A000050/1) Centre for Interventional and Surgical Sciences, University College London. HM is also funded by the NIHR Biomedical Research Centre at University College London. DK is supported by an NIHR Academic Clinical Fellowship. DK is also supported by a Cancer Research UK Predoctoral Fellowship. For the purpose of Open Access, the authors have applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials