

Neurofilament light chain marks severity of papilledema in idiopathic intracranial hypertension
- PMID: 36689008
- PMCID: PMC10175309
- DOI: 10.1007/s10072-023-06616-z
Neurofilament light chain marks severity of papilledema in idiopathic intracranial hypertension
Abstract
Background: Neurofilament light chain (NfL) reflects axonal damage in neurological disorders. It has recently been evaluated in idiopathic intracranial hypertension (IIH). A biomarker indicating the severity of optic nerve damage in IIH could support diagnostic accuracy and therapeutic decisions.
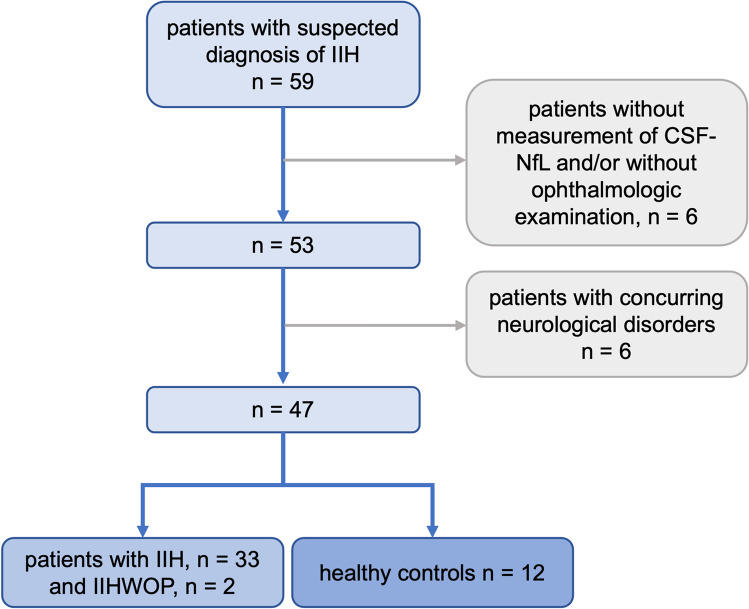
Methods: We retrospectively reviewed NfL concentrations in the cerebrospinal fluid (CSF) of 35 IIH patients and 12 healthy controls, who had received diagnostic workup for IIH in our clinic. The diagnosis of IIH was made according to the modified Friedman criteria for IIH and for IIH without papilledema Friedman DI et al Neurol 81:1159-1165 (2013) [1]. NfL in the CSF (CSF-NfL) was correlated with the severity of papilledema and with CSF opening pressure.
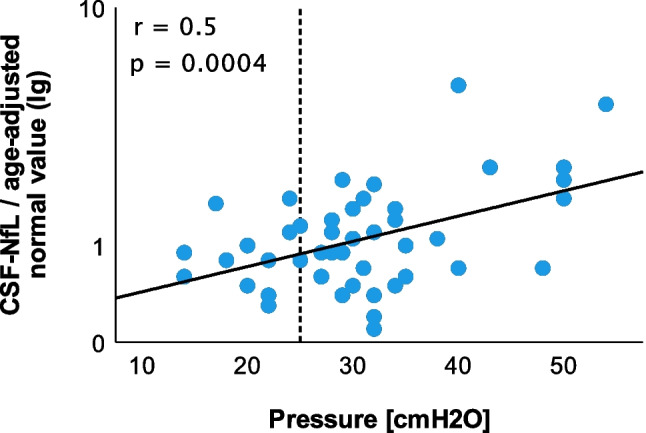
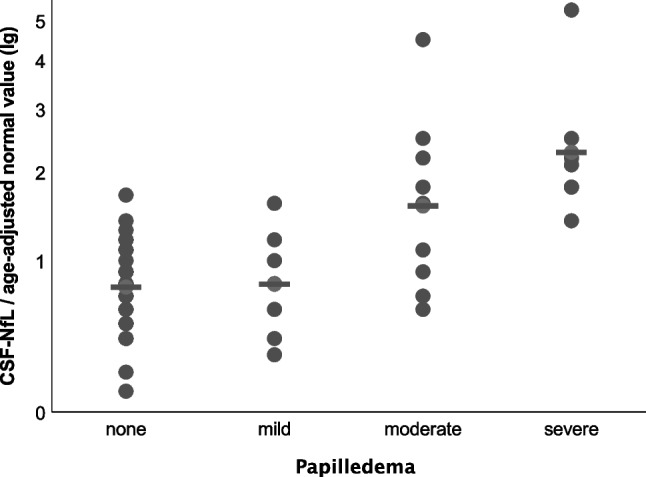
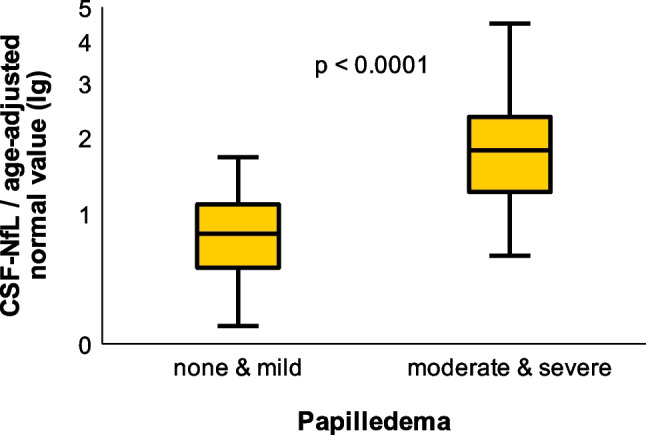
Results: CSF-NfL correlated with CSF opening pressure at the time of collection. In patients with IIH and moderate or severe papilledema, CSF-NfL was significantly increased compared to patients with mild or no papilledema. Healthy controls with raised intracranial pressure showed no relevant elevation of CSF-NfL.
Conclusion: CSF-NfL appears to correlate with the severity of papilledema in IIH and with CSF opening pressure and may therefore be a predictor of optic nerve damage in IIH patients.
Keywords: CSF opening pressure; Idiopathic intracranial hypertension; Neurofilament light chain; Papilledema.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no financial or non-financial conflicts of interest to disclose. The authors are indebted to the patients for their participation in this study.
Figures
Similar articles
-
Elevated neurofilament light chain CSF/serum ratio indicates impaired CSF outflow in idiopathic intracranial hypertension.Fluids Barriers CNS. 2023 Jan 11;20(1):3. doi: 10.1186/s12987-022-00403-2. Fluids Barriers CNS. 2023. PMID: 36631830 Free PMC article.
-
Optic Nerve Angle in Idiopathic Intracranial Hypertension.J Neuroophthalmol. 2021 Dec 1;41(4):e464-e469. doi: 10.1097/WNO.0000000000000986. J Neuroophthalmol. 2021. PMID: 34788243
-
The Pre-Lumbar puncture Intracranial Hypertension Scale (PLIHS): A practical scale to identify subjects with normal cerebrospinal fluid pressure in the management of idiopathic intracranial hypertension.J Neurol Sci. 2021 Oct 15;429:118058. doi: 10.1016/j.jns.2021.118058. Epub 2021 Aug 27. J Neurol Sci. 2021. PMID: 34461550
-
Papilledema: A review of etiology, pathophysiology, diagnosis, and management.Surv Ophthalmol. 2022 Jul-Aug;67(4):1135-1159. doi: 10.1016/j.survophthal.2021.11.007. Epub 2021 Nov 20. Surv Ophthalmol. 2022. PMID: 34813854 Review.
-
Expanding the clinical spectrum of idiopathic intracranial hypertension.Curr Opin Neurol. 2023 Feb 1;36(1):43-50. doi: 10.1097/WCO.0000000000001131. Epub 2022 Nov 28. Curr Opin Neurol. 2023. PMID: 36444979 Free PMC article. Review.
Cited by
-
Predicting Outcomes of Preterm Neonates Post Intraventricular Hemorrhage.Int J Mol Sci. 2024 Sep 25;25(19):10304. doi: 10.3390/ijms251910304. Int J Mol Sci. 2024. PMID: 39408633 Free PMC article.
-
Neurofilament Light Chain Concentration in Cerebrospinal Fluid in Children with Acute Nontraumatic Neurological Disorders.Children (Basel). 2024 Mar 19;11(3):360. doi: 10.3390/children11030360. Children (Basel). 2024. PMID: 38539395 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
