

Removal of the magnetic sphincter augmentation device: an assessment of etiology, clinical presentation, and management
- PMID: 36689039
- PMCID: PMC10156860
- DOI: 10.1007/s00464-023-09878-y
Removal of the magnetic sphincter augmentation device: an assessment of etiology, clinical presentation, and management
Abstract
Background: Magnetic sphincter augmentation (MSA) erosion, disruption or displacement clearly requires device removal. However, up to 5.5% of patients without anatomical failure require removal for dysphagia or recurrent GERD symptoms. Studies characterizing these patients or their management are limited. We aimed to characterize these patients, compare their outcomes, and determine the necessity for further reflux surgery.
Methods: This is a retrospective review of 777 patients who underwent MSA at our institution between 2013 and 2021. Patients who underwent device removal for persistent dysphagia or recurrent GERD symptoms were included. Demographic, clinical, objective testing, and quality of life data obtained preoperatively, after implantation and following removal were compared between removal for dysphagia and GERD groups. Sub-analyses were performed comparing outcomes with and without an anti-reflux surgery (ARS) at the time of removal.
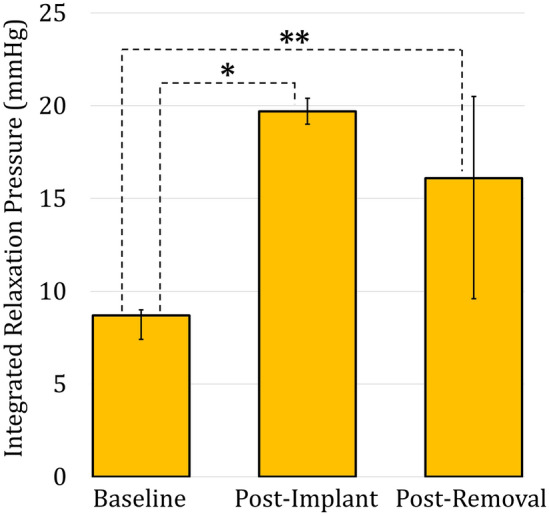
Results: A total of 40 (5.1%) patients underwent device removal, 31 (77.5%) for dysphagia and 9 (22.5%) for GERD. After implantation, dysphagia patients had less heartburn (12.9-vs-77.7%, p = 0.0005) less regurgitation (16.1-vs-55.5%, p = 0.0286), and more pH-normalization (91.7-vs-33.3%, p = 0.0158). Removal without ARS was performed in 5 (55.6%) GERD and 22 (71.0%) dysphagia patients. Removal for dysphagia patients had more complete symptom resolution (63.6-vs-0.0%, p = 0.0159), freedom from PPIs (81.8-vs-0.0%, p = 0.0016) and pH-normalization (77.8-vs-0.0%, p = 0.0455). Patients who underwent removal for dysphagia had comparable symptom resolution (p = 0.6770, freedom from PPI (p = 0.3841) and pH-normalization (p = 0.2534) with or without ARS. Those who refused ARS with removal for GERD had more heartburn (100.0%-vs-25.0%, p = 0.0476), regurgitation (80.0%-vs-0.0%, p = 0.0476) and PPI use (75.0%-vs-0.0%, p = 0.0476).
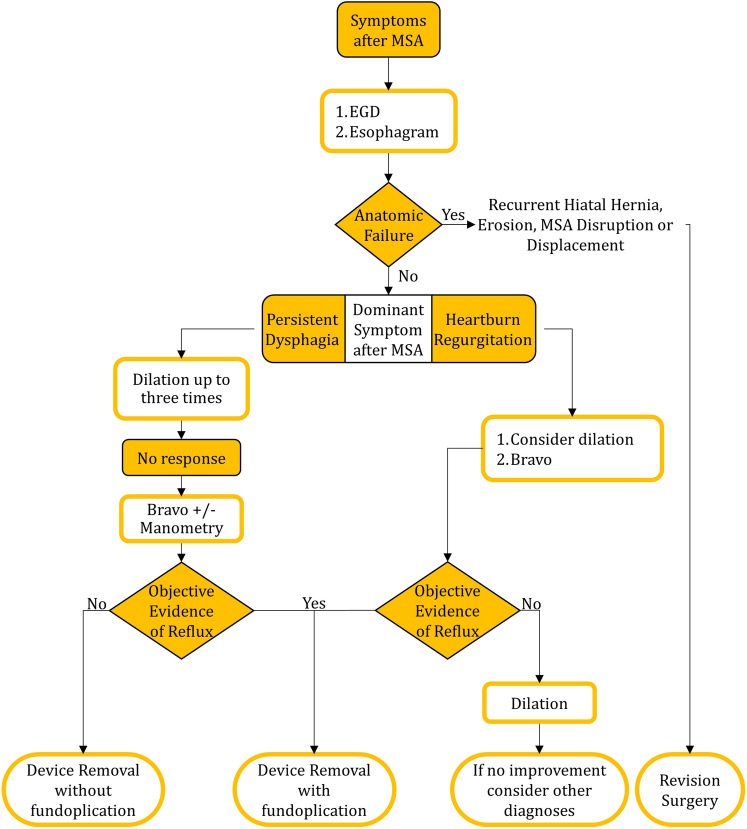
Conclusions: MSA removal outcomes are dependent on the indication for removal. Removal for dysphagia yields excellent outcomes regardless of anti-reflux surgery. Patients with persistent GERD had worse outcomes on all measures without ARS. We propose a tailored approach to MSA removal-based indication for removal.
Keywords: Device removal; Dysphagia; Gastroesophageal reflux disease; Magnetic sphincter augmentation; Symptom recurrence.
© 2023. The Author(s).
Conflict of interest statement
SA and BJ: serve on the scientific advisory board of Johnson and Johnson and receive a consulting fee. SE, KS, TH and PZ have no conflicts of interest or financial disclosures. Authors SE, KS, SA, TH, PZ, BAJ have no conflicts of interest or financial ties to disclose.
Figures
Similar articles
-
Need for frequent dilations after magnetic sphincter augmentation: an assessment of associated factors and outcomes.Surg Endosc. 2023 Sep;37(9):7159-7169. doi: 10.1007/s00464-023-10197-5. Epub 2023 Jun 19. Surg Endosc. 2023. PMID: 37336846
-
One hundred consecutive patients treated with magnetic sphincter augmentation for gastroesophageal reflux disease: 6 years of clinical experience from a single center.J Am Coll Surg. 2013 Oct;217(4):577-85. doi: 10.1016/j.jamcollsurg.2013.04.039. Epub 2013 Jul 12. J Am Coll Surg. 2013. PMID: 23856355
-
S148: Long-term patient-reported outcomes of laparoscopic magnetic sphincter augmentation versus Nissen fundoplication: a 5-year follow-up study.Surg Endosc. 2022 Sep;36(9):6851-6858. doi: 10.1007/s00464-022-09015-1. Epub 2022 Jan 18. Surg Endosc. 2022. PMID: 35041056
-
Laparoscopic magnetic sphincter augmentation versus fundoplication for gastroesophageal reflux disease: systematic review and pooled analysis.Dis Esophagus. 2019 Nov 13;32(9):doz031. doi: 10.1093/dote/doz031. Dis Esophagus. 2019. PMID: 31069388
-
MAGNETIC SPHINCTER AUGMENTATION DEVICE FOR GASTROESOPHAGEAL REFLUX DISEASE: EFFECTIVE, BUT POSTOPERATIVE DYSPHAGIA AND RISK OF EROSION SHOULD NOT BE UNDERESTIMATED. A SYSTEMATIC REVIEW AND META-ANALYSIS.Arq Bras Cir Dig. 2024 Mar 4;36:e1781. doi: 10.1590/0102-672020230063e1781. eCollection 2024. Arq Bras Cir Dig. 2024. PMID: 38451590 Free PMC article.
Cited by
-
Impact of Change in Sizing Protocol on Outcome of Magnetic Sphincter Augmentation.Ann Surg. 2025 Mar 1;281(3):454-461. doi: 10.1097/SLA.0000000000006249. Epub 2024 Feb 23. Ann Surg. 2025. PMID: 38390758 Free PMC article.
-
The failure pattern for the magnetic sphincter augmentation device: a single-institution case series with literature review.Surg Endosc. 2025 Aug;39(8):4956-4964. doi: 10.1007/s00464-025-11842-x. Epub 2025 Jun 26. Surg Endosc. 2025. PMID: 40571793 Free PMC article. Review.
-
Safety profile of magnetic sphincter augmentation for gastroesophageal reflux disease.Front Surg. 2023 Nov 7;10:1293270. doi: 10.3389/fsurg.2023.1293270. eCollection 2023. Front Surg. 2023. PMID: 38026489 Free PMC article.
References
-
- Bonavina L, DeMeester T, Fockens P, Dunn D, Saino G, Bona D, Lipham J, Bemelman W, Ganz RA. Laparoscopic sphincter augmentation device eliminates reflux symptoms and normalizes esophageal acid exposure: one- and 2-year results of a feasibility trial. Ann Surg. 2010;252:857–862. doi: 10.1097/SLA.0b013e3181fd879b. - DOI - PubMed
-
- Ayazi S, Zheng P, Zaidi AH, Chovanec K, Salvitti M, Newhams K, Hoppo T, Jobe BA. Clinical outcomes and predictors of favorable result after laparoscopic magnetic sphincter augmentation: single-institution experience with more than 500 patients. J Am Coll Surg. 2020;230:733–743. doi: 10.1016/j.jamcollsurg.2020.01.026. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
